Introduction
Palmar fasciitis with polyarthritis (PFPA) has a
characteristics clinical course that involves rapidly bilateral
arthritis of the hands and fasciitis of the palms (1,2). This
results in pain, swelling and progressive contractures of the
hands. These symptoms can co-occur with less severe synovitis of
distant articilations. The palmar skin generally shows nodular
erythema, and nodularity of the flexor tendons is often noted. This
is a rare disease, while it is important for physicians to be able
to recognize the disease in the patients with theses characteristic
clinical symptoms and screen for malignancy (3–5).
Extensive review of underlying malignancies associated with PFPA
showed ovarian cancer accounting for the majority (37%) of the
cases (6).
In the all patients from case series and single case
reports described, the ovarian cancer is already present in an
advanced stage. We attempted to present our case and systemically
review available evidence on the association between PFPA and
ovarian cancer, as gynecological oncologists.
Case report
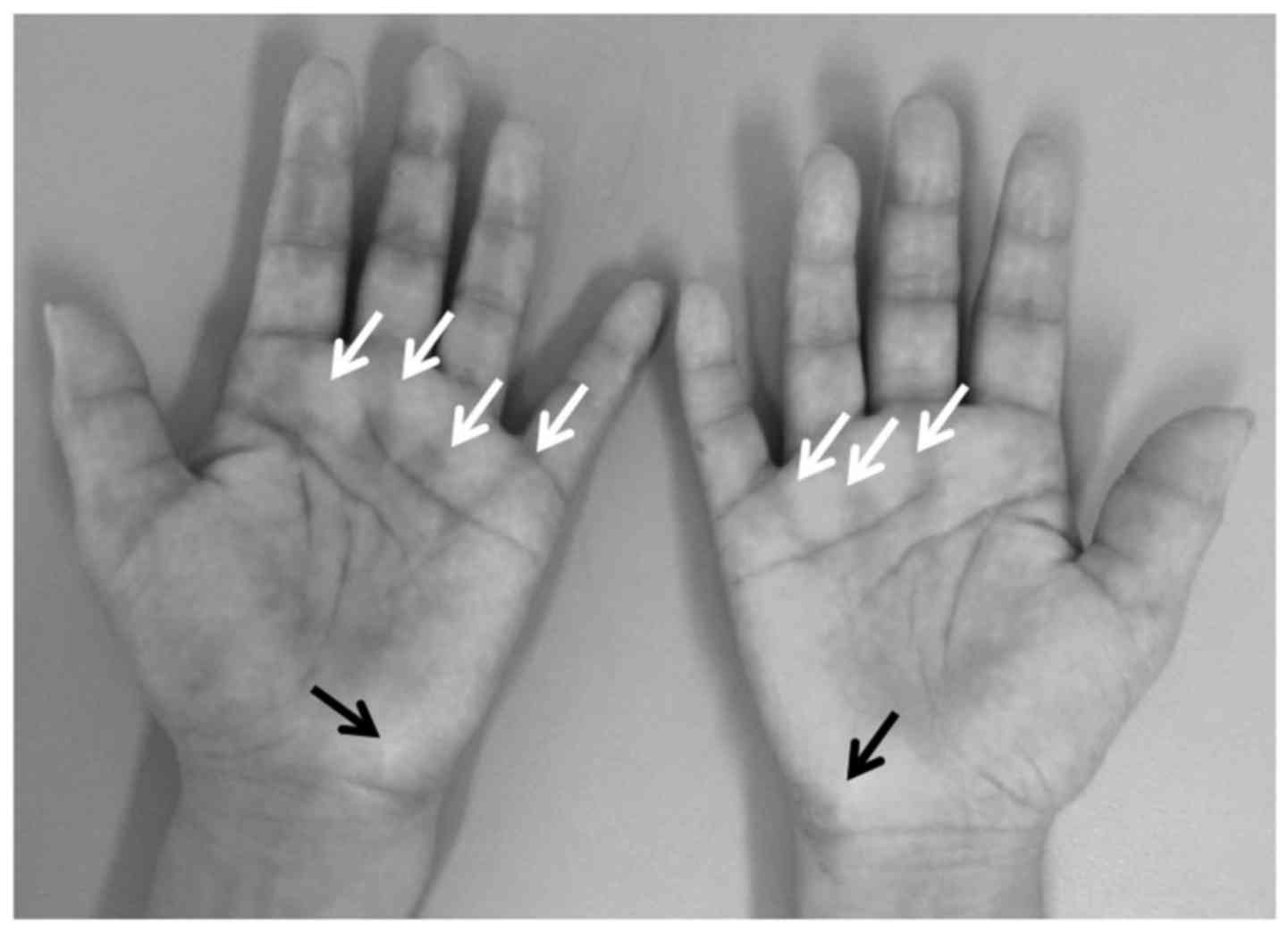
A 61-year-old woman presented with a 1-year history
of bilateral progressive painful swelling of the hands (Fig. 1) with stiffness and diffuse
arthralgia in the elbows and knees. In addition, a half-year after
the onset, she suffered from fatigue and reported a weight loss of
2 kg within the last 1-month. There was no improvement with
predonisone (15 mg/day). Laboratory tests revealed a normal
complete blood count, sedimentation rate, and routine chemistry
results. Antinuclear antibody, extractable nuclear antigen
antibodies, anti-citrulinated peptide antibodies and rheumatoid
factor testing were normal. Magnetic resonance imaging (MRI) showed
high-intensity nodules above the flexor tendons. However, there was
no evidence of MRI findings suggestive of the existence of
arthritis.
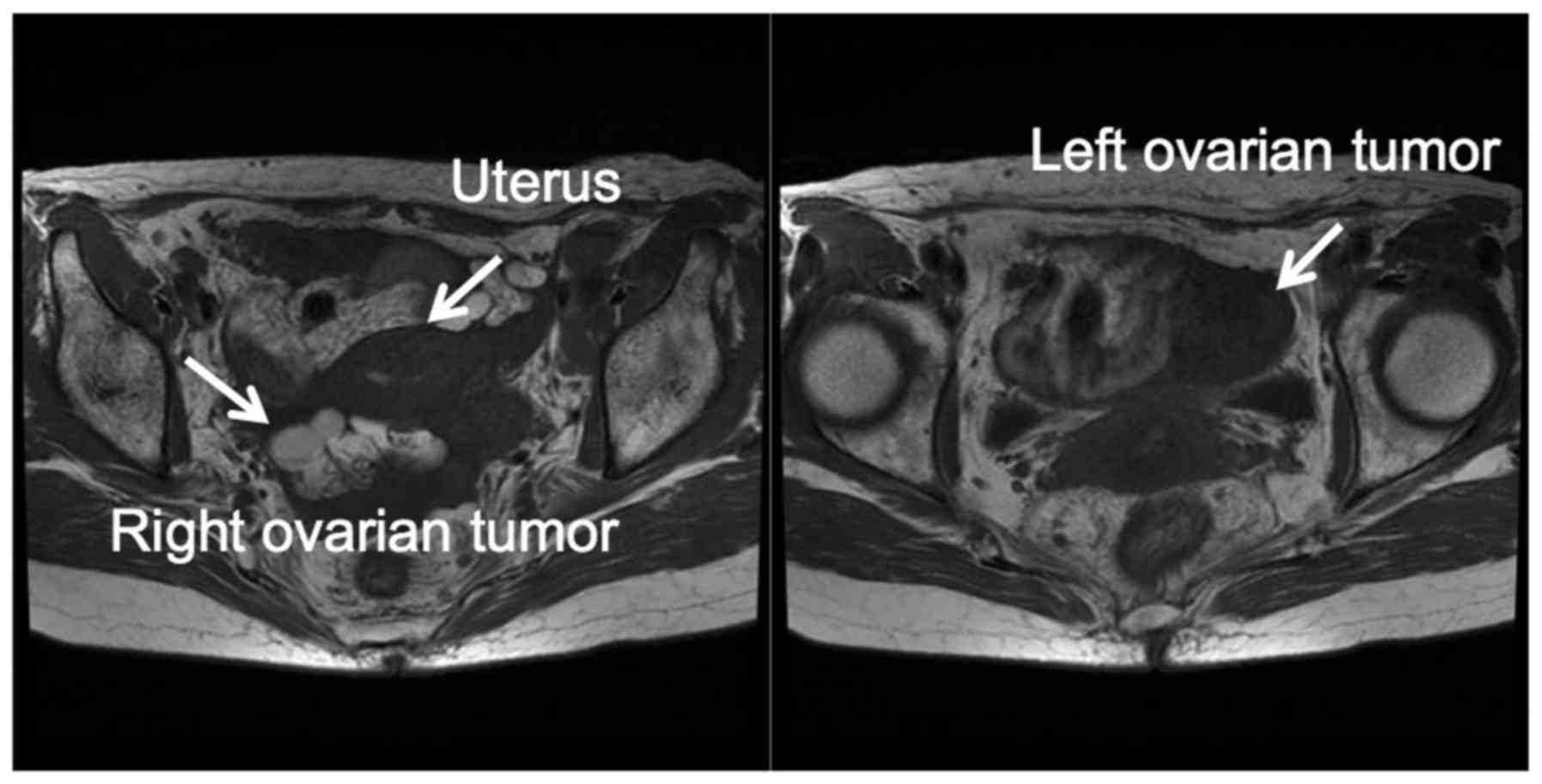
Consideration of the unusual clinical findings and
the progressive palmar contracture led to possible diagnosis of
palmar fasciitis. The cancer-associated disease (6–8) prompted
us to screen the most frequent underlying malignancy including
ovarian cancer. Abdominal MRI showed a mass of the bilateral ovary
with signs of peritoneal and omental metastases (Fig. 2).
The patient was submitted to exploratory laparotomy.
There was a sold, gray and brown mixed mass (5 cm) in the left
ovary, widespread malignant deposits (<2 cm) within the pelvis,
and omental fullness due to metastatic tumor. The right ovary was
involved. A complete staging with hysterectomy, bilateral
salpingo-ophorectomy, omentectomy was performed. Histological
examination of the tissue revealed a poorly differentiated serous
adenocarcinoma originated from left ovary with omental involvement
and peritoneal dissemination. Cytology of ascites yielded poorly
differentiated adenocarcinoma. The stage was IIIB (pT3BNxM0). The
patient was expected to receive postoperative chemotherapy with
carboplatin and paclitaxel. Although the patient is still under
intensive chemotherapy, the dismal prognosis of this condition
prompted us to review our experience with PFPA associated ovarian
cancer and previous literatures. The patient provided written
informed consent to study publication.
Literature review of PFPA-associated ovarian
cancer
In a literature review we found 17 case series and
single case reports of PFPA associated ovarian and fallopian
cancers (Table I). The association
between the malignancies and a PFPA condition has been dominantly
in the elderly. Their age of previously reported patients was
postmenopausal women, except younger 2 cases (25 and 42 years).
 | Table I.Fallopian tube and ovarian cancers
related palmar fasciitis with polyarthritis. |
Table I.
Fallopian tube and ovarian cancers
related palmar fasciitis with polyarthritis.
| First author,
year | Age (years) | Histology | Stage | (Refs.) |
|---|
| A, Fallopian
tube |
|
| Fukui, 2015 | 64a | Serous
adenocarcinoma | pT3cNxM0 | (11) |
| Taggart, 1984 | 58 | Well differentiated
adenocarcinoma | Not described
(peritoneal spread) | (10) |
| Denschlag, 2004 | 73 | Serous papillary
adenocarcinoma | Not described
(complete staging surgery performed) withpartial rejection of colon
due to tumor infiltration | (9) |
|
| B, Ovary |
|
| Medsger, 1982 | 6 postmenopausal (50
to 65) | Endometrial
carcinoma, G2 or G3 | Non-resectable tumor
and peritoneal seeding in all patients. | (23) |
| Martorell, 2004 | 4 postmenopausal (51
to 73) | Serous papillary
adenocarcinoma pT3CN0M0 and 1 of pT3BN0M0 | 2 of pT4NxM1, 1
of | (24) |
| Taggart, 1984 | 42 | Poorly differentiated
adenocarcinoma | Not described
(peritoneal spread) | (10) |
| Yogarajah, 2008 | 74 | Poorly differentiated
adenocarcinoma | Not described
(peritoneal spread) | (25) |
| Preda, 2009 | 62 | Poorly differentiated
adenocarcinoma | Inoperable | (16) |
| Strobel, 1992 | 59 | Serous
adenocarcinoma | pT3CN1M0 | (26) |
| Salmon, 2013 | 2 postmenopausal (58
and 69) | Serous adenocarcinoma
and adenocarcinoma | pT3BN0M0 and T3CNxM0
(not operated) | (27) |
| Pfinsgraff, 1986 | 57 | Adenocarcinoma | T4NxM1 | (28) |
| Bremer, 1967 | 50 | Not identified | T4NxM1 | (29) |
| Van Marcke, 2017 | 70 | Serous
adenocarcinoma | pT3CN1M0 | (21) |
| Qureshi, 2011 | 73 | Serous
adenocarcinoma | pT3CNxM0 | (7) |
| Manger, 2014 | 73 | Serous
adenocarcinoma | pT3CNxM0 | (6) |
| Vinker, 1996 | 25 | Serous papillary
adenocarcinoma | Stage IV | (30) |
| Shiel, 1985 | 75 | Serous
adenocarcinoma | Stage IV | (31) |
|
| 61 | Serous
adenocarcinoma | pT3BNxM0 | Present case |
In over 60% of all cases, by far the most frequently
occurring histological type was serous (papillary) adenocarcinoma.
The poorly differentiated or undifferentiated adenocarcinoma
accounted for 25%, and the characterized as endometrioid only in
one report (6 cases). All patients were diagnosed already in
advanced stage of metastatic spreading.
PFPA symptoms preceded the diagnosis of ovarian
cancer, or PFPA symptoms led to immediate detection of an
underlying these cancers. Interestingly in 2 cases of 3 fallopian
tube cancers, the diagnosis of underlying malignancies by
laparotomy preceded the onset of PFPA symptoms by 1 year (9,10). In
another case of fallopian tube cancer, the diagnosis of PFPA led to
the immediate detection of an underlying malignancy (11). There are many similarities between
fallopian tube cancer and ovarian cancer, and ovarian cancer is
believed to originate in the distal and proximal fallopian tube
(12–15). Research published over the past 10
years has suggested that the most ‘ovarian cancer’, and
specifically the high-grade serous carcinoma subtype of ovarian
cancer, actually originates in the fallopian tube (13,15).
PFPA-associated fallopian tube cancer may be the precursor of at
least ovarian serous adenocarcinoma of the ovary.
The pathophysiology of PFPA is unclear. One
hypothesis involves abnormalities in humoral and immune responses
associated with the malignancy and responsible for overproduction
of certain cytokines (16,17). Considering all reported
cancer-associated syndromes and associated cancer, the majority of
affected patients have been elderly women, which suggests the
female hormone state may predispose to this syndrome as is the case
in most autoimmune disease. The cytokines [e.g., vascular
endothelial growth factor (VEGF), insulin-like growth factor (IGF),
transforming growth factor β (TGF-β)] play an important role in
ovarian stromal proliferation and emergence of ovarian cancer
(18–20). Ovarian cancer and fallopian tube
cancer release many types of cytokines such as VEGF, IGF, TGF-β
(20). A higher level of TGF-β and
VEGF may be a candidate to facilitate the rapid progression in the
patients with PFPA associated with malignancies.
Treatment of the underlying cancer is paramount to
the management of PFPA symptoms. Almost half of the patients
reported describe a decrease in the symptoms after surgery,
chemotherapy and/or radiotherapy (6,21). The
role of new biological agents, such as TGF inhibitors and VEGF
inhibitors, in this indication remains unclear, but their
immunosuppressive and anti-angiogenic properties could
theoretically be detrimental and trigger cancer progression.
Ovarian benign tumors
PFPA has been implicated also with ovarian
non-malignant tumors including endometrial cyst (1) and paraovarian cyst (22). As PFPA was suspected, a more complete
investigation was performed in these 2 cases. Abdominal imaging
demonstrated a pelvic cystic mass rising from adnexa. Currently
there are no effective screening methods for ovarian cancer and the
malignancies frequently remains undiagnosed until metastasis has
occurred. When found in PFPA patients, the ovarian tumor highly
suspected as benign should be removed and submitted to pathological
examination.
Comments
Learning PFPA and its presentations in particular by
gynecologic oncologist can rise the suspicion of underlying
ovarian/fallopian cancer. The commitment of the attending
physicians to become familiar with and identify rare disease may
lead to the detection at an early and curative stage. As the
symptoms of PFPA can usually precede cancer detection, and are
unrelated to tumor stage, rapid diagnosis of PFPA can expedite
effective management of the malignancy. Currently there are no
effective screening methods for ovarian cancer and the malignancies
frequently remains undiagnosed until advance stage. We recommend a
thorough malignancy work-up by gynecological oncologist for any
women presenting with the sudden onset of unexplained hand pain,
inflammatory fasciitis, or palmar fibromatosis.
References
|
1
|
Champion GD, Saxon JA and Kossard S: The
syndrome of palmar fibromatosis (fasciitis) and polyarthritis. J
Rheumatol. 14:1196–1198. 1987.PubMed/NCBI
|
|
2
|
Alexandroff AB, Hazleman BL, Matthewson M,
Black CM, Rytina E, Crawford R and Burrows NP: Woody hands. Lancet.
361:13442003. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Haroon M and Phelan M: A paraneoplastic
case of palmar fasciitis and polyarthritis syndrome. Nat Clin Pract
Rheumatol. 4:274–277. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Azar L and Khasnis A: Paraneoplastic
rheumatologic syndromes. Curr Opin Rheumatol. 25:44–49. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Baron M: Palmar fasciitis, polyarthritis
and carcinoma. Ann Intern Med. 97:6161982. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Manger B and Schett G: Palmar fasciitis
and polyarthritis syndrome-systematic literature review of 100
cases. Semin Arthritis Rheum. 44:105–111. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Qureshi AA and Saavedra A: Palmar
fasciitis and polyarthritis syndrome in patients with ovarian
cancer-a case report and review of the literature. Hand(N Y).
6:220–223. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Scheinfeld N: A review of the cutaneous
paraneoplastic associations and metastatic presentations of ovarian
carcinoma. Clin Exp Dermatol. 33:10–15. 2008.PubMed/NCBI
|
|
9
|
Denschlag D, Riener E, Vaith P, Tempfer C
and Keck C: Palmar fasciitis and polyarthritis as a paraneoplastic
syndrome associated with tubal carcinoma: A case report. Ann Rheum
Dis. 63:1177–1178. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Taggart AJ, Iveson JM and Wright V:
Shoulder-hand syndrome and symmetrical arthralgia in patients with
tubo-ovarian carcinoma. Ann Rheum Dis. 43:391–393. 1984. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Fukui S, Fujiwara S, Kobayashi S, Kamei S,
Takizawa Y, Setoguchi K, Uno M and Funata N: Fallopian tube cancer
with palmar fibromatosis or fasciitis without polyarthritis. Intern
Med. 54:2409–2414. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Carlson JW, Miron A, Jarboe EA, Parast MM,
Hirsch MS, Lee Y, Muto MG, Kindelberger D and Crum CP: Serous tubal
intraepithelial carcinoma: Its potential role in primary peritoneal
serous carcinoma and serous cancer prevention. J Clin Oncol.
26:4160–4165. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Dietl J: Revisiting the pathogenesis of
ovarian cancer: The central role of the fallopian tube. Arch
Gynecol Obstet. 289:241–246. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Lee Y, Miron A, Drapkin R, Nucci MR,
Medeiros F, Saleemuddin A, Garber J, Birch C, Mou H, Gordon RW, et
al: A candidate precursor to serous carcinoma that originates in
the distal fallopian tube. J Pathol. 211:26–35. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Reade CJ, McVey RM, Tone AA, Finlayson SJ,
McAlpine JN, Fung-Kee-Fung M and Ferguson SE: The fallopian tube as
the origin of high grade serous ovarian cancer: Review of a
paradigm shift. J Obstet Gynaecol Can. 36:133–140. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Preda V, Frederiksen P and Kossard S:
Indurated reticulate palmar erythema as a sign of paraneoplastic
palmar fasciitis and polyarthritis syndrome. Australas J Dermatol.
50:198–201. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Mehra S, Walker J, Patterson K and
Fritzler MJ: Autoantibodies in systemic sclerosis. Autoimmun Rev.
12:340–354. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Emori C and Sugiura K: Role of
oocyte-derived paracrine factors in follicular development. Anim
Sci J. 85:627–633. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Geva E and Jaffe RB: Role of vascular
endothelial growth factor in ovarian physiology and pathology.
Fertil Steril. 74:429–438. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Imai A, Ichigo S, Matsunami K, Takagi H
and Kawabata I: Ovarian function following targeted anti-angiogenic
therapy with bevacizumab. Mol Clin Oncol. 6:807–810. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
van Marcke C, Seront E, Docquier C and
Filleul B: Palmar fasciitis and polyarthritis, a rare
paraneoplastic syndrome related to ovarian cancer. Clin Exp
Dermatol. 42:328–330. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Fernandez-Nebro A, Fernandez-Ruiz A,
Rodriguez M, Haro M, Rodriguez-Andreu J and Gonzalez-Santos P:
Palmar fasciitis and polyarthritis syndrome is multicausal. Clin
Rheumatol. 15:99–101. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Medsger TA, Dixon JA and Garwood VF:
Palmar fasciitis and polyarthritis associated with ovarian
carcinoma. Ann Intern Med. 96:424–431. 1982. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Martorell EA, Murray PM, Peterson JJ,
Menke DM and Calamia KT: Palmar fasciitis and arthritis syndrome
associated with metastatic ovarian carcinoma: A report of four
cases. J Hand Surg Am. 29:1–660. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Yogarajah M, Soh J, Lord B, Goddard N and
Stratton R: Palmar fasciitis and polyarthritis syndrome: A sign of
ovarian malignancy. J R Soc Med. 101:473–475. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Strobel ES, Lacour M and Peter HH: Palmar
fascial thickening and contractures of fingers resembling
arthritis-a paraneoplastic symptom? Rheumatol Int. 12:79–80. 1992.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Salmon C, Gill G, Loeuille D and
Chary-Valckenaere I: Three new cases of palmar fasciitis with
polyarthritis including a patient with atypical mutilating
osteolysis. Joint Bone Spine. 80:217–220. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Pfinsgraff J, Buckingham RB, Killian PJ,
Keister SR, Brereton WF, Weinblatt ME, George DL and Arnett FC:
Palmar fasciitis and arthritis with malignant neoplasms: A
paraneoplastic syndrome. Semin Arthritis Rheum. 16:118–125. 1986.
View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Bremer C: Shoulder-hand syndrome. A case
of unusual aetiology. Ann Phys Med. 9:168–171. 1967.PubMed/NCBI
|
|
30
|
Vinker S, Dgani R, Lifschitz-Mercer B,
Sthoeger ZM and Green L: Palmar fasciitis and polyarthritis
associated with ovarian carcinoma in a young patient. A case report
and review of the literature. Clin Rheumatol. 15:495–497. 1996.
View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Shiel WJ, Prete PE, Jason M and Andrews
BS: Palmar fasciitis and arthritis with ovarian and non-ovarian
carcinomas. New syndrome. Am J Med. 79:640–644. 1985. View Article : Google Scholar : PubMed/NCBI
|