Introduction
There has been growing interest in the effects of
magnetic fields (MFs) on cancer research and therapy in recent
years. Huang et al (1)
investigated the effects of 20-mT, 50-Hz sinusoidal MFs on cell
proliferation, ion concentration and osmolarity in two human cancer
cell lines (HL-60 and SK-Hep-1). MFs inhibition of cell growth was
observed and the authors concluded that these inhibitions in
vitro may relate to changes in cell ion concentration and
osmolarity. A synergistic effect was found when immunocompetent
mice bearing murine Lewis lung carcinomas (LLCs) or B16 melanotic
melanomas treated with cisplatin were exposed to extremely
low-frequency (ELF)-MFs (2).
Novikov et al (3) suggested
that MFs have a marked antitumor activity. Mice with transplanted
Ehrlich ascites carcinoma (EAC) were exposed to weak MFs and the
tumor tissue was almost completely absent after exposure. Zhang
et al (4) reported that ELF
pulsed-gradient MFs induce apoptosis of cancer cells and arrest
neoangiogenesis, inhibiting murine malignant tumor growth.
The mechanism of the anticancer activity of MFs is
uncertain. Ronchetto et al (5) hypothesized that the free radical
recombination processes were influenced by MFs, which activated p53
gene-dependent survival mechanisms. Elson (6) reported the production of numerous
breaks in DNA and the overwhelming of DNA repair processes, leading
to the apoptotic process. DNA damage was also considered as one of
the possible mechanisms. Ruiz-Gómez and Martínez-Morillo (7) reviewed 29 studies and concluded that
MFs act as co-inductors of DNA damage.
Certain researchers have evaluated the toxicity of
MFs. Tofani S et al (2)
reported that no clinical signs or toxicity were observed in any
mice exposed to MFs compared with mice administered
cyclophosphamide or cisplatin. Sprague-Dawley rats were exposed to
20 kHz triangular MFs in the study of Lee et al (8) and the authors concluded that MFs did
not increase toxicity in rats. In clinical research, Ronchetto
et al (5) assessed acute
toxicity in patients with advanced neoplasia who accepted static
MFs treatment and concluded that MFs may be safely administrated
according to the exposure schedules.
In vivo and in vitro, the inhibition
of MFs on tumor cell proliferation has been reported in numerous
studies (9–12). However, thus far, clinical trials to
evaluate the improvement of survival and general symptoms in
advanced cancer patients treated with ELF-MFs have not been
performed. Therefore, 13 advanced non-small cell lung cancer
(NSCLC) patients were enrolled in this study. The aim of this study
was to investigate the efficacy and safety of ELF-MFs in patients
with advanced NSCLC and measure the improvement of survival and
general symptoms in patients.
Subjects and methods
Patient eligibility
Between August 2007 and September 2010, 13 patients
with histologically or cytologically confirmed locally advanced or
metastatic NSCLC (disease stage IV) were considered as candidates
in this pilot study. Patients who enrolled in this study were in
accordance with the eligibility criteria listed in Table I: expected survival time ≥2 months,
Karnofsky performance status (KPS) score between 30 and 60%, not
pregnant or children and disease stage IV according to the UICC TNM
classification. Previous therapy, including surgery, chemotherapy,
radiation therapy or combined treatment, were not included in the
eligibility criteria, but patients must not have received these
therapies for at least 1 month prior to enrollment in this study
and have abandoned treatment after their disease recurred to be
involved in this study. There were also requirements concerning the
function of certain organs; patients with severe arrest of bone
marrow (grade 3–4) were excluded, adequate hepatic and renal
function were required and patients with severe heart disease were
excluded.
 | Table IPatient eligibility criteria. |
Table I
Patient eligibility criteria.
| Histologically or
cytologically confirmed NCSLC |
| Disease stage IV,
according to the UICC TNM classification |
| Karnofsky
performance status score 30–60% |
| Patients or their
family members abandoned treatment after disease recurrence |
| Expected survival
time ≥2 months |
| Appropriate
hepatic, heart and renal function |
| No severe arrest of
bone marrow (grade 3–4) |
| Informed
consent |
| No pregnant females
or children |
The research procedures were performed with the
consent of the patients and ethics committee approval and were in
accordance with the Helsinki Declaration of 1975, as revised in
1983.
Treatment schedule
The MFs exposure generated by permanent magnets was
employed. The system was designed by Shandong Chaoruishi Medical
Science and Technology Company (Zibo, China) and is a static MFs
device, which consists of two magnetic heads. In each magnetic
head, a pair of fan-shaped NdFeB permanent magnets, which generate
MFs, are located on a circular iron plate. The two magnetic heads
rotate together around the patient. The bottom magnetic head is
driven by an electro-motor, while the bonding force of the bottom
magnetic head causes the top magnet to rotate synchronously. The
MFs of the device are alternative pulses which are regulated from
0.38 to 0.42 T. The rotation speed of the magnetic heads is
regulated from 300 to 600 r/min. The frequency of the MFs was 0–50
Hz. The treatment bed was made of plexiglass located between the
two magnetic heads.
When treatment started, patients laid on the
treatment bed of the ELF-MFs machine. The area of treatment
included the primary tumor site, metastatic sites and metastatic
lymph nodes. The treatment schedule was as follows: subjects were
exposed to 420 r/min, 0.4-T MFs, 2 h per day, 5 days per week for
6–10 weeks.
Toxicity and side-effects were evaluated according
to WHO criteria. Before and following ELF-MFs treatment, all 13
patients underwent clinical tests, including physical examination,
routine analysis of blood, ECG and liver function, biochemical and
kidney function tests in order to evaluate toxicity and
side-effects of ELF-MFs. During the treatment process, patients
were observed to determine whether they had severe side-effects. If
intolerable side-effects were reported, the treatment was
stopped.
Changes in general symptoms, including pleural
effusion, shortness of breath, cancer pain, appetite, physical
capacity, constipation and insomnia, were recorded during ELF-MFs
treatment and 2 weeks after the completion of therapy.
Follow-up
The follow-up methods included outpatient service
and telephone interview. Following ELF-MFs treatment, all 13
patients were followed up every 3 months in the first year and
every 6 months in the second and third year until the mortality of
the patient. The last date of follow-up was September 20, 2010.
Statistical analysis
Survival time was calculated from the end of
treatment to mortality or last follow-up and was expressed as
months. Overall survival, the 1- and 2-year survival rates and
mortality or last follow-up results were evaluated by the
Kaplan-Meier method. Overall survival was measured from the date of
completion of ELF-MFs treatment to the date of mortality or last
follow-up. Data analyses were conducted with SPSS 17.0 statistical
software package (SPSS, Inc., Chicago, IL, USA). P<0.05 was
considered to indicate a statistically significant result.
Results
Patient characteristics
Of these 13 subjects, 5 were female and 8 were male
and the median age was 65 years (range, 51–85). The characteristics
of the patients are summarised in Table
II. All patients suffered locally advanced or metastatic
disease. Of these patients, 5 had single-site metastasis (lung,
bone, liver and peritoneal cavity), 3 had multi-site metastases and
5 had no metastasis. Before the study, a total of 5 patients had
not received anti-tumor treatment and 8 patients had received
treatment, including chemotherapy, surgery or combined treatment.
All the subjects experienced recurrence, and they abandoned
treatment before receiving ELF-MFs.
| Table IICharacteristics of NSCLC
patients. |
Table II
Characteristics of NSCLC
patients.
|
Characteristics | Number (n=13) |
|---|
| Age (years), median
(range) | 65 (51–85) |
| Gender, n (%) | |
| Male | 8 (61.5) |
| Female | 5 (38.5) |
| Previous therapy, n
(%) | |
| Chemotherapy
only | 5 (38.5) |
| Surgery only | 1 (7.7) |
| Combined
treatment | 2 (15.4) |
| None | 5 (38.5) |
| Site of metastasis,
n (%) | |
| Lung | 1 (7.7) |
| Bone | 2 (15.3) |
| Liver | 1 (7.7) |
| Peritoneal
cavity | 1 (7.7) |
| Multi-site
metastases | 3 (23.1) |
| None | 5 (38.5) |
Palliation of general symptoms
After the treatment, the clinical symptoms of all
patients were investigated. The improvement of the general symptoms
of all subjects are shown in Table
III. Before ELF-MFs treatment, 2 patients had pleural effusion
and a decrease in pleural effusion was observed in these cases at
the end of treatment. A total of 5 patients reported remission of
shortness of breath in the post-treatment period compared with
pre-therapy of ELF-MFs. A total of 5 patients reported that
magnetic treatment relieved cancer pain to various degrees. Lack of
appetite is common in patients with advanced neoplasia; 6 patients
in this study stated that they had increased appetite after
treatment. One patient each reported constipation and irregular
bowel movement before the treatment, and their bowel habit became
regular, with once every 1–2 and 2–3 days, respectively, following
treatment. Other clinical symptoms, including improved physical
strength and better sleep quality, were detected in 9 and 1
patients, respectively. During the ELF-MFs treatment, 2 patients
presented with improved symptoms during therapy, while the
palliation of symptoms disappeared at treatment termination.
| Table IIISymptom improvement of NSCLC
patients. |
Table III
Symptom improvement of NSCLC
patients.
| Variable | Number (%) |
|---|
| Pleural effusion
decreasing | 2 (15.4) |
| Remission of
shortness of breath | 5 (38.5) |
| Relief of cancer
pain | 5 (38.5) |
| Increased
appetite | 6 (46.2) |
| Improved physical
strength | 9 (69.2) |
| Better sleep
quality | 1 (7.7) |
| Regular bowel
movement | 2 (15.4) |
| Palliation of
symptomsa | 2 (15.4) |
Toxicity and side-effects
Grades 1 and 2 arrest of bone marrow was detected in
2 (15.4%) patients and 1 (7.7%) patient, respectively. Increased
heart rate of 3–5 bpm was observed in 2 (15.4%) patients. There was
an increase of temperature of 0.5–1.0˚C in 3 (23.1%) patients
(Table IV). No severe side-effects
or toxicity were detected in the 13 advanced NSCLC patients treated
by ELF-MFs in our trial.
| Table IVToxicity and side-effects in NSCLC
patients. |
Table IV
Toxicity and side-effects in NSCLC
patients.
| Variable | Number (%) |
|---|
| Grade 1 arrest of
bone marrow | 2 (15.3) |
| Grade 2 arrest of
bone marrow | 1 (7.7) |
| Increased heart
rate of 3–5 bpm | 2 (15.4) |
| Increased
temperature of 0.5–1.0˚C | 3 (23.1) |
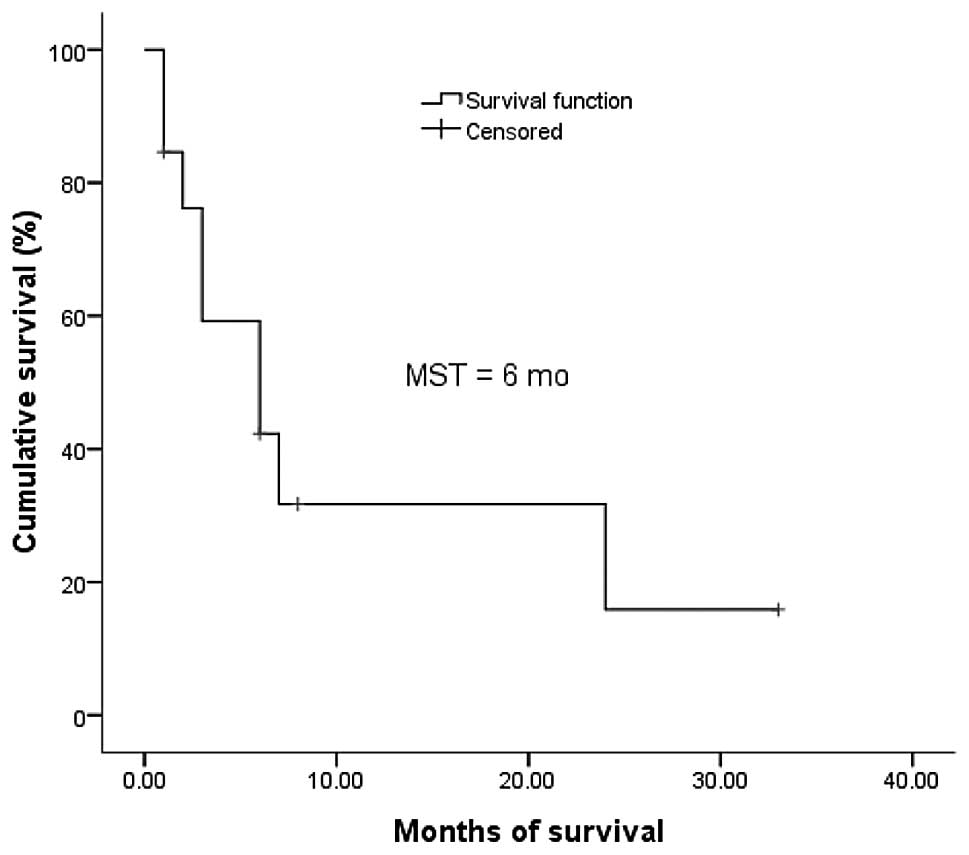
Survival analysis
The 13 patients were all followed up either for 33
months or until mortality. The follow-up rate was 100.0%. At the
end of follow-up, 9 patients had succumbed to the disease, 1
patient was lost to follow-up and 3 patients were still alive. The
median survival was 6.0 months (95% CI, 1.0–11.0). The 1- and
2-year survival rates were 31.7 and 15.9%, respectively (Fig. 1).
Discussion
Lung cancer is one of the most common malignancies
worldwide, both in incidence and mortality, and is the leading
cause of cancer-related mortality in the world (13,14).
NSCLC accounts for approximately 80% of all lung tumors, 65–80% of
which present as locally advanced or metastatic disease (15). For locally advanced or metastatic
lung cancer, treatment is limited. Surgical excision is impossible
in most patients, while supportive care and chemotherapy is widely
used (14). Chemotherapy, either
first- or second-line regimen, has low response rates and a high
incidence of side-effects, which affect quality of life (QOL)
outcomes of advanced or metastatic lung cancer patients (16,17).
MFs may be useful for the improvement of general symptoms and QOL
outcomes of patients. It has been reported that MFs with specific
physical characteristics may be safely used to treat patients with
advanced neoplasia, and the patients have a good tolerability
(5,9).
We reviewed the English language literature and
found that studies mainly focused on basic experimental studies,
while only one clinical study was found to assess the safety of MFs
treatment for patients with cancer (5). However, at present, no clinical trial
to investigate the effects of ELF-MFs on survival and palliation of
general symptoms in patients with advanced neoplasia has been
performed. The aim of this study was to evaluate the improvement of
general symptoms and survival in 13 advanced NSCLC patients treated
by ELF-MFs.
Our results showed that the median survival was 6.0
months (95% CI, 1.0–11.0). A meta-analysis (18) reported that the median survival of
the advanced NSCLC patients receiving supportive care was 4.0
months. This study demonstrated that the median survival of
patients treated with ELF-MFs was longer than that of those
receiving supportive care. Our median survival of 6.0 months was
less than that of 9.1 and 8.4 months of cisplatin- and
carboplatin-treated advanced NSCLC patients, respectively (19). Furthermore, the 1-year survival rate
was 31.7 in our ELF-MFs trial, which was lower than the 37 and 34%
reoprted in cisplatin- and carboplatin-treated patients (19). However, the 1-year survival rate in
ELF-MFs-treated advanced NSCLC patients was higher than that
reported in the meta-analysis (18), whose 1-year survival rate in
patients who received supportive care was 15%. The median survival
and 1-year survival rate of ELF-MFs-, supportive care, cisplatin-
and carboplatin-treated patients are listed in Table V. According to the comparison of the
median survival and the 1-year survival rate between ELF-MFs and
supportive care treatments, we conclude that the advanced NSCLC
patients may benefit from ELF-MFs treatment. Although the median
survival and the 1-year survival rate in the ELF-MFs trial is no
more than that of chemotherapy treatment (18–20),
there are lower levels of toxicity and excellent tolerability in
patients treated with ELF-MFs. In chemotherapy treatment for
advanced NSCLC patients, toxicity includes neutropenia,
thrombocytopenia, diarrhea, nausea, vomiting and fatigue (16,17,21,22).
However, in our trial, 2 (15.4%) patients had grade 1 arrest of
bone marrow and 1 (7.7%) patient had grade 2. Increased heart rate
of 3–5 bpm and temperature increase of 0.5–1.0˚C was observed in 2
(15.4%) and 3 (23.1%) patients, respectively. We concluded that no
severe toxicity or side-effects were detected in ELF-MFs treatment,
which was in accordance with previous studies (5).
| Table VMedian survival and 1-year survival
rate of ELF-MFs-, supportive care, cisplatin- and
carboplatin-treated patients. |
Table V
Median survival and 1-year survival
rate of ELF-MFs-, supportive care, cisplatin- and
carboplatin-treated patients.
| Variable | Median survival
(months) | 1-year survival
rate (%) |
|---|
| ELF-MFs | 6.0 | 31.7 |
| Supportive
carea | 4.0 | 15.0 |
|
Cisplatin-treatedb | 9.1 | 37.0 |
|
Carboplatin-treatedb | 8.4 | 34.0 |
For advanced, especially stage IV, NSCLC patients in
our trial, the chance of attaining complete remission was limited.
It was essential to prolong survival (16) and improve general symptoms, which
may lead to improvement of QOL in these patients. However,
chemotherapy-induced side-effects remain a significant clinical
problem in advanced NSCLC (16). It
has been previously documented that cancer patients who undergo
chemotherapy experience treatment-related symptoms and
side-effects, including nausea, insomnia, diarrhea and diminished
physical capacity (16,17,21,22).
By contrast, in the ELF-MFs treatment, the patients showed
improvements in pleural effusion, shortness of breath, cancer pain,
appetite, physical capacity, bowel movement and sleep quality in a
certain number of patients. This finding demonstrates that ELF-MFs
may moderately improve general symptoms in advanced NSCLC.
In conclusion, the results of our pilot trial with a
small number of patients suggest that ELF-MFs may be an effective,
well-tolerated and safe method of treatment of advanced NSCLC to
prolong survival and moderately improve general symptoms. This is
the first study to describe survival and palliation of general
symptoms and the results merit further studies.
Acknowledgements
This study was supported by the
program of ‘Science and Technology Development Plan of Shandong
Province of China’ (No. 2011GSF11843).
References
|
1.
|
L HuangL DongY ChenH QiD XiaoEffects of
sinusoidal magnetic field observed on cell proliferation, ion
concentration, and osmolarity in two human cancer cell
linesElectromagn Biol
Med25113126200610.1080/1536837060071906716771300
|
|
2.
|
S TofaniD BaroneM BerardelliE BernoM
CintorinoL FogliaP OssolaF RonchettoE TosoM EandiStatic and ELF
magnetic fields enhance the in vivo anti-tumor efficacy of
cis-platin against lewis lung carcinoma, but not of
cyclophosphamide against B16 melanotic melanomaPharmacol
Res4883902003
|
|
3.
|
VV NovikovGV NovikovEE FesenkoEffect of
weak combined static and extremely low-frequency alternating
magnetic fields on tumor growth in mice inoculated with the Ehrlich
ascites
carcinomaBioelectromagnetics30343351200910.1002/bem.20487
|
|
4.
|
X ZhangH ZhangC ZhengC LiX ZhangW
XiongExtremely low frequency (ELF) pulsed-gradient magnetic fields
inhibit malignant tumour growth at different biological levelsCell
Biol Int26599603200210.1006/cbir.2002.088312127939
|
|
5.
|
F RonchettoD BaroneM CintorinoM
BerardelliS LissoloR OrlassinoP OssolaS TofaniExtremely low
frequency-modulated static magnetic fields to treat cancer: A pilot
study on patients with advanced neoplasm to assess safety and acute
toxicityBioelectromagnetics25563571200410.1002/bem.20029
|
|
6.
|
E ElsonI. The little explored efficacy of
magnetic fields in cancer treatment and postulation of the
mechanism of actionElectromagn Biol
Med28275282200910.3109/1536837090311427120001703
|
|
7.
|
MJ Ruiz-GómezM
Martínez-MorilloElectromagnetic fields and the induction of DNA
strand breaksElectromagn Biol Med28201214200919811402
|
|
8.
|
HJ LeeYM GimmHD ChoiN KimSH KimYS
LeeChronic exposure of Sprague-Dawley rats to 20 kHz triangular
magnetic fieldsInt J Radiat
Biol86384389201010.3109/0955300090356792020397843
|
|
9.
|
T WangY NieS ZhaoY HanY DuY HouInvolvement
of midkine expression in the inhibitory effects of low-frequency
magnetic fields on cancer
cellsBioelectromagnetics32443452201110.1002/bem.2065421360556
|
|
10.
|
R de SezeS TuffetJM MoreauB VeyretEffects
of 100 mT time varying magnetic fields on the growth of tumors in
miceBioelectromagnetics21107111200010653621
|
|
11.
|
S TofaniD BaroneM CintorinoMM de SantiA
FerraraR OrlassinoP OssolaF PeroglioK RolfoF RonchettoStatic and
ELF magnetic fields induce tumor growth inhibition and
apoptosisBioelectromagnetics22419428200110.1002/bem.6911536283
|
|
12.
|
T HisamitsuK NaritaT KasaharaA SetoY YuK
AsanoInduction of apoptosis in human leukemic cells by magnetic
fieldsJpn J Physiol47307310199710.2170/jjphysiol.47.3079271162
|
|
13.
|
Z HuX ChenY ZhaoT TianG JinY ShuY ChenL
XuK ZenC ZhangH ShenSerum microRNA signatures identified in a
genome-wide serum microRNA expression profiling predict survival of
non-small-cell lung cancerJ Clin
Oncol2817211726201010.1200/JCO.2009.24.934220194856
|
|
14.
|
G GaoH ChuL ZhaoT GuiQ XuJ ShiA
meta-analysis of paclitaxel-based chemotherapies administered once
every week compared with once every 3 weeks first-line treatment of
advanced non-small-cell lung cancerLung
Cancer76380386201210.1016/j.lungcan.2011.12.00122226626
|
|
15.
|
S NovelloT Le ChevalierChemotherapy for
non-small-cell lung cancer. Part 1: Early-stage diseaseOncology
(Williston Park)17357364200312661267
|
|
16.
|
L GuoSP BaiL ZhaoXH WangAstragalus
polysaccharide injection integrated with vinorelbine and cisplatin
for patients with advanced non-small cell lung cancer: effects on
quality of life and survivalMed OncolSep182011(E-pub ahead of
print)
|
|
17.
|
L AdamsenM QuistJ MidtgaardC AndersenT
MøllerL KnutsenA TveteråsM RorthThe effect of a multidimensional
exercise intervention on physical capacity, well-being and quality
of life in cancer patients undergoing chemotherapySupport Care
Cancer14116127200610.1007/s00520-005-0864-x
|
|
18.
|
No authors listed: Chemotherapy in
non-small cell lung cancer: a meta-analysis using updated data on
individual patients from 52 randomised clinical trials. Non-small
Cell Lung Cancer Collaborative
GroupBMJ311899909199510.1136/bmj.311.7010.899
|
|
19.
|
A ArdizzoniL BoniM TiseoFV FossellaJH
SchillerM PaesmansD RadosavljevicA PaccagnellaP ZatloukalP
MazzantiD BissetR RosellCISCA (CISplatin versus CArboplatin)
Meta-analysis Group: Cisplatin-versus carboplatin-based
chemotherapy in first-line treatment of advanced non-small-cell
lung cancer: an individual patient data meta-analysisJ Natl Cancer
Inst99847857200710.1093/jnci/djk196
|
|
20.
|
A ChiapporiG BeplerF BarlesiJC SoriaM
ReckA BearzF BarataG ScagliottiK ParkA WagleAM LiepaYD ZhaoN
ChouakiN IscoeJ von PawelPhase II, double-blinded, randomized study
of enzastaurin plus pemetrexed as second-line therapy in patients
with advanced non-small cell lung cancerJ Thorac
Oncol5369375201010.1097/JTO.0b013e3181cee24f20090562
|
|
21.
|
WX QiZ ShenY YaoMeta-analysis of
docetaxel-based doublet versus docetaxel alone as second-line
treatment for advanced non-small-cell lung cancerCancer Chemother
Pharmacol6999106201210.1007/s00280-011-1678-921607554
|
|
22.
|
WX QiLN TangAN HeZ ShenY YaoEffectiveness
and safety of pemetrexed-based doublet versus pemetrexed alone as
second-line treatment for advanced non-small-cell lung cancer: a
systematic review and meta-analysisJ Cancer Res Clin
Oncol138745751201210.1007/s00432-012-1155-922258853
|