Introduction
The incidence of follicular thyroid cancer is lower
than that of papillary thyroid cancer in thyroid malignant tumors
and is, therefore, the second most common thyroid malignancy
(1). Follicular thyroid cancer is
mainly characterized by a follicular structure. It is a
differentiated thyroid cancer and demonstrates positive expression
of the sodium-iodide symporter. Therefore, the tissues of
follicular thyroid cancer generally uptake iodine, which is the
biological basis for the detection of cancer lesions by
131I whole-body imaging and the treatment of follicular
thyroid cancer by radioactive 131I (2,3).
99mTcO4− and the iodide ion have a
number of similar features, so
99mTcO4− can also be absorbed by
the thyorid (4). Follicular thyroid
cancer may develop into regional nodal metastasis and may also
progress into hematogenous metastasis (1). The accurate detection of recurrent and
metastatic lesions of follicular thyroid cancer is significant in
the staging of diseases and the evaluation of the therapeutic
effect and prognosis (1). The
present study describes a patient with follicular thyroid cancer
whose metastatic lesions were detected using a
99mTcO4− whole-body scan. Informed
consent was obtained from the patient prior to the study.
Case report
A 69-year-old female was admitted to Zhongnan
Hospital of Wuhan University (Hubei, China) complaining of left
stethalgia for three weeks. A physical examination revealed that
the second rib in anterior left chest and the fourth thoracic
vertebra were swollen and painful when palpated. The thyroid glands
of the patient were intumescent and the left lobe to the isthmic
portion was palpated as a hard and fixed nodule with an asperous
surface, without pain. Laboratory examination demonstrated that the
thyroid, liver and kidney functions, as well as the routine blood
and urine test results, were all normal.
Thyroid imaging was performed at 10 min following
the intravenous injection of Na99mTcO4 at 185
MBq. The result demonstrated a regional area of markedly decreased
99mTcO4− uptake with an irregular
edge within the middle portion of the left lobe of the thyroid. A
conglomerate area of increased
99mTcO4− uptake was identified in
the left chest (Fig. 1).
Subsequently, 99mTcO4− whole-body
imaging was performed for the patient. The result revealed abnormal
lesions of increased 99mTcO4−
uptake in the left chest, thoracic vertebrae, lumbar vertebrae and
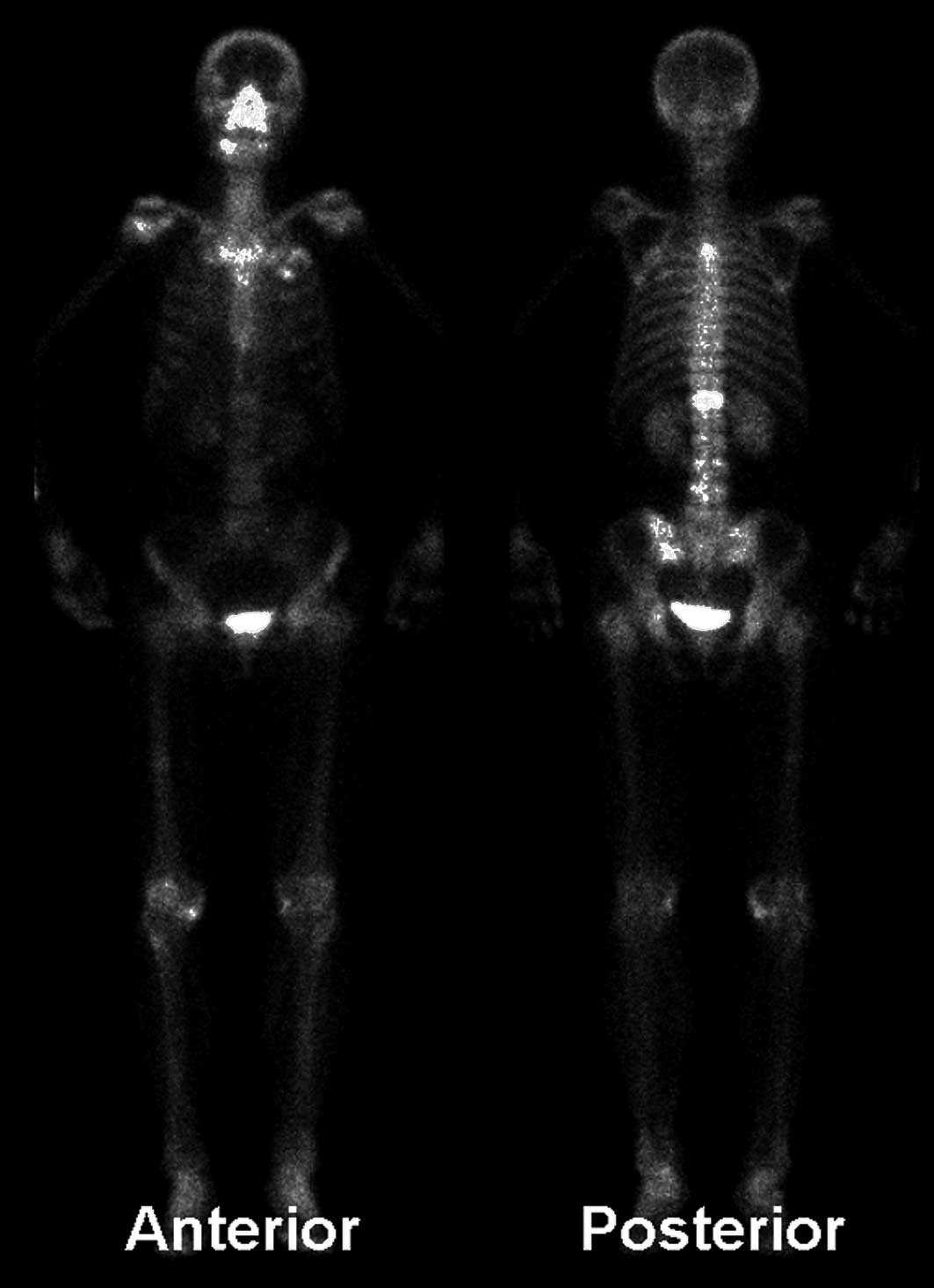
left ilium (Fig. 2). The following
day, whole-body bone imaging was performed at 3 h following an
intravenous injection of 99mTc-methylene diphosphonate
at 740 MBq. The imaging outcome demonstrated that the left anterior
branch of the second rib, the fourth and twelfth thoracic vertebrae
and the midpiece of the right thigh bone exhibited increased
radioactive uptake. The third and fourth lumbar vertebrae and the
left posterior inferior iliac spine were suspected of abnormal
uptake, whereas the partial osseous tissue of the left anterior
branch of the second rib demonstrated decreased radioactive uptake
(Fig. 3).
A computed tomography (CT) scan of the thoracic
region revealed a mass on the left thoracic wall, bony destruction
of the left anterior branch of the second rib (Fig. 4) and the destruction of the crest of
the fourth thoracic vertebra (Fig.
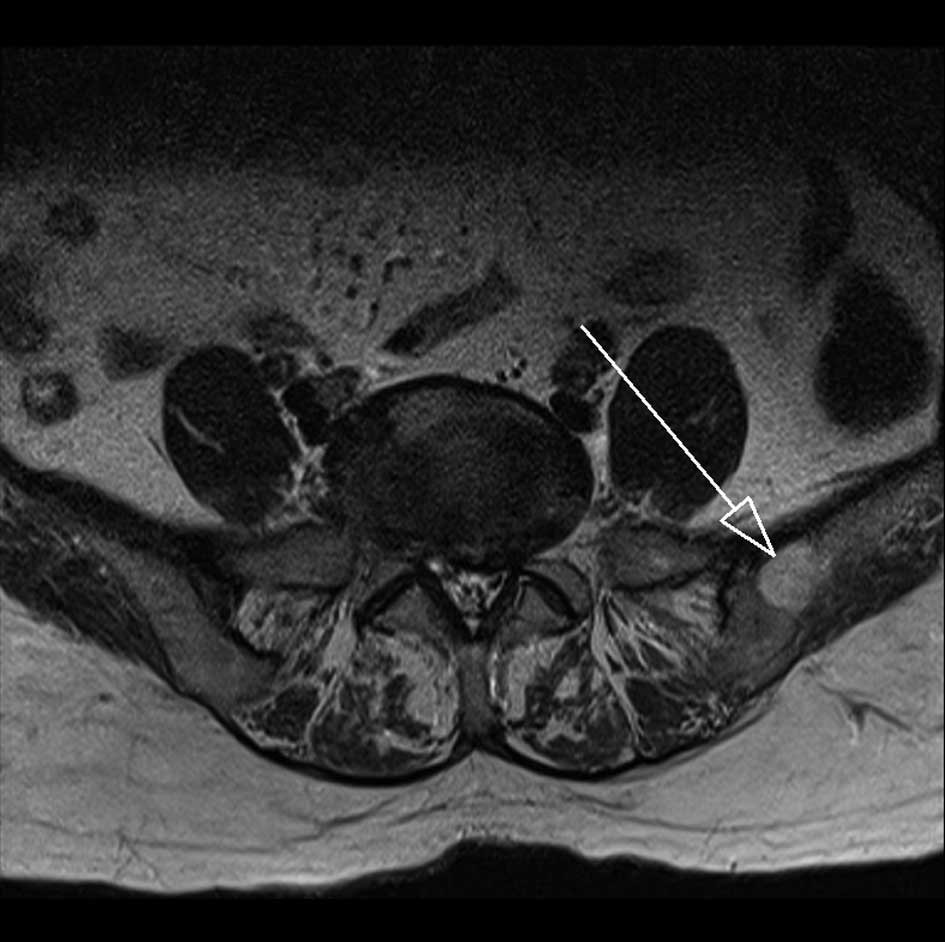
5). A magnetic resonance imaging (MRI) scan of the vertebrae
and pelvic cavity demonstrated that the twelfth thoracic vertebra
(Figs. 6 and 7), the pedicle of the fourth lumbar
vertebral arch (Fig. 7) and the
left ilium presented an abnormal signal (Fig. 8).
The patient underwent a total thyroidectomy. The
pathological results revealed that the left lobe nodule of thyroid
was composed of follicular thyroid cancer tissue with peplos
infiltration and tumor embolus formation of the small vessels.
Discussion
131I whole-body imaging is often used for
the identification of metastatic lesions of differentiated thyroid
cancer following total thyroidectomy (2,3). When
thyroid tissues are not completely resected, 131I is
largely absorbed by the existing normal thyroid tissues (5). However, metastatic lesions universally
have a low uptake of 131I and, therefore, the metastatic
lesions are not displayed clearly (5). As a result, 131I whole-body
imaging is not generally selected to identify the metastatic
lesions of thyroid cancer in the presence of normal thyroid
tissues. 99mTcO4− is similar to
the iodide ion to a certain extent (4);
99mTcO4− and the iodide ion are
mediated by the sodium-iodide symporter and are absorbed by thyroid
follicular cells (4). Therefore,
the two methods are often used in thyroid imaging (6). However, 99mTcO4
imaging is not generally used to detect the metastatic lesions of
thyroid cancer in the presence of thyroid tissues and also
following a total thyroidectomy (6–8).
Follicular thyroid cancer tissues are mainly
composed of differentiated follicular cells. The proteins of the
sodium-iodide symporter are predominantly distributed in the
membrane of follicular epithelial cells, and cancer tissues with
follicular cells express sodium-iodide symporter proteins (9,10),
which are the pacing factors for which 131I and
99mTcO4− are absorbed by the
cancer tissues. The quantity of cancer tissues absorbing
99mTcO4− correlates with the level
of sodium-iodide symporter protein expression. Since cancer tissues
are not well-differentiated, the level of sodium-iodide symporter
protein expression is low (10,11).
Accordingly, the lesions of thyroid cancer frequently manifest
‘cool nodules’ or ‘cold nodules’ of decreased
99mTcO4− uptake (12). When thyroid tissues are not operated
on, an increased 99mTcO4− uptake
of metastatic lesions of thyroid cancer is rare. Certain studies
have reported an increased uptake of neck metastases of thyroid
cancer in 99mTcO4− thyroid imaging
(7,8,13–15).
However, to the best of our knowledge, there have been no studies
with regard to the increased uptake of whole-body multiple
metastatic lesions of thyroid cancer in
99mTcO4− whole-body imaging. The
present study incidentally identified a mass outside of the thyroid
gland in a patient with thyroid ‘cool nodules’, which exhibited
increased 99mTcO4− uptake in the
routine image field. Subsequently, a whole-body scan was performed.
The result demonstrated that similar lesions of increased
99mTcO4− uptake existed in
multiple positions of the whole body. CT, MRI and radionuclide
whole-body bone imaging confirmed that the multitudinous sites of
increased uptake, which were detected by
99mTcO4− imaging, contained tumor
lesions. Therefore, despite the fact that
99mTcO4− imaging is not routinely
used to identify metastatic lesions of thyroid cancer, when
regional lesions of increased
99mTcO4− uptake are observed
outside of the thyroid glands during routine field thyroid static
imaging, further identification of the metastatic lesions of the
whole body is significant.
Furthermore,
99mTcO4− whole-body imaging has
numerous advantages. The procedure is highly sensitive, as shown by
the third and fourth lumbar vertebral lesions and the ilium lesion,
which were detected by 99mTcO4−
imaging, but were not observed on the whole-body bone scan. MRI
only identified the lesions of the fourth lumbar vertebra and the
ilium, but not the third lumbar vertebral lesion. These results
indicate that the sensitivity of
99mTcO4− whole-body imaging is
higher than that of MRI and whole-body bone scan at this time.
Furthermore, the procedure is highly specific. The fact that
99mTcO4− was able to be absorbed
by thyroid cancer tissues under the mediation of sodium-iodide
symporter proteins, confirms the diagnostic specificity for
regional lesions. Abnormally increased
99mTcO4− uptake of the lesions
outside of the thyroid glands is a characteristic of metastatic
thyroid cancer tissues (7,8,13–15),
suggesting that the lesions likely originated from thyroid tissues.
Finally, the procedure increases the quality of the diagnosis of
the thyroid nodules. For the patient of the present study, the
feature of the ‘cool nodule’ was not enough to discriminate between
malignant lesions and benign tumors. However, the identification of
the metastatic lesions extremely supported the diagnosis of the
malignant thyroid nodule. The
99mTcO4− imaging examination is
able to scan the whole body of patients and, therefore, the
detection area is extensive, which conduces to a complete detection
of the lesions.
References
|
1
|
Grebe SK and Hay ID: Follicular thyroid
cancer. Endocrinol Metab Clin North Am. 24:761–801. 1995.
|
|
2
|
Muresan MM, Olivier P, Leclère J, et al:
Bone metastases from differentiated thyroid carcinoma. Endocr Relat
Cancer. 15:37–49. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Krishna L, Dadparvar S, Brady LW, et al:
Paradoxical changes in iodine-131 scintigraphic findings in
advanced follicular thyroid cancer. J Nucl Med. 34:1574–1576.
1993.PubMed/NCBI
|
|
4
|
Zuckier LS, Dohan O, Li Y, Chang CJ,
Carrasco N and Dadachova E: Kinetics of perrhenate uptake and
comparative biodistribution of perrhenate, pertechnetate, and
iodide by NaI symporter-expressing tissues in vivo. J Nucl Med.
45:500–507. 2004.PubMed/NCBI
|
|
5
|
Tian R, Kuang AR, Qin WS and Zhang HM:
Value of post-therapy whole-body 131I scan in the
evaluation of patients with differentiated thyroid cancer. Chin J
Nucl Med. 20:162–164. 2000.(In Chinese).
|
|
6
|
Haugen BR and Lin EC: Isotope imaging for
metastatic thyroid cancer. Endocrinol Metab Clin North Am.
30:469–492. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Mathiopoulou L, Chrisoulidou A, Boudina M,
Mitsakis P, Mandanas S and Pazaitou-Panayiotou K: 99mTc
pertechnetate thyroid scan leads to serendipitous detection of
metastatic thyroid cancer. Clin Nucl Med. 37:604–606. 2012.
View Article : Google Scholar
|
|
8
|
Campbell CM and Khafagi FA: Insensitivity
of Tc-99m pertechnetate for detecting metastases of differentiated
thyroid carcinoma. Clin Nucl Med. 15:1–4. 1990. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Wang SS, Liang J, Lin YS and Yao RY:
Differential expression of the Na symporter protein in thyroid
cancer and adjacent normal and nodular goiter tissues. Oncol Lett.
5:368–372. 2012.PubMed/NCBI
|
|
10
|
Liou MJ, Lin JD, Chan EC, Liu FH, Chao TC
and Weng HF: Detection of mRNA of sodium iodide symporter in benign
and malignant human thyroid tissues. Cancer Lett. 160:75–80. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Peyrottes I, Navarro V, Ondo-Mendez A, et
al: Immunoanalysis indicates that the sodium iodide symporter is
not overexpressed in intracellular compartments in thyroid and
breast cancers. Eur J Endocrinol. 60:215–225. 2009.PubMed/NCBI
|
|
12
|
Summaria V, Rufini V, Mirk P, Costantini
AM, Reale F and Maresca G: Diagnostic imaging of differentiated
thyroid carcinoma. Rays. 25:177–190. 2000.(In English,
Italian).
|
|
13
|
Krausz Y and Horne T: Detection of
metastatic thyroid carcinoma by 99mTc-pertechnetate in the presence
of hyperfunctioning thyroid tissue. J Surg Oncol. 44:132–134. 1990.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Kumaresan K and Sastry RA: Localization of
Tc-99m pertechnetate in lymph node metastasis from occult thyroid
carcinoma. Clin Nucl Med. 19:11121994. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Khan SU, Khan AU, Khan A, Shah AS and Khan
K: Extrathyroidal uptake from thyroid carcinoma on
99mTc-pertechnetate scintigraphy. J Coll Physicians Surg
Pak. 21:772–774. 2011.PubMed/NCBI
|