Introduction
Primary cardiac tumors are rare, as demonstrated by
their low frequency (0.001–0.03%) in an autopsy series (1,2), which
indicated that 15–25% of the primary cardiac tumors were malignant
(3,4). Sarcomas comprised two-thirds of these
malignancies. The sarcoma subtypes, known as angiosarcomas and
myxofibrosarcomas, are the most common cardiac sarcomas. Notably, a
cardiac osteosarcoma is extremely rare (3–8).
Surgical resection is the preferred treatment option for this type
of sarcoma; however, even with surgical treatment, patients
generally have a poor prognosis, with the median overall survival
ranging from 6 to 12 months (5,8–10). An
important and critical factor related to the severity of the
prognosis, is the occurrence of distant metastasis. Bakaeen et
al (11) reported that even if
a partial surgical resection is performed, the combination of
surgical resection and radio- and/or chemotherapy is effective
(11). To the best of our
knowledge, there have been no previous reports regarding the
resection of a metastatic rectal tumor originating from an
osteosarcoma of the heart and there are no published guidelines for
the treatment of metastatic sarcomas in the intestine. The present
case study discusses a patient who underwent a laparoscopic
resection of a metastatic osteosarcoma in the rectum originating
from the heart.
Case report
A 41-year-old male was admitted to the Osaka Medical
Center for Cancer and Cardiovascular Diseases (Osaka, Japan) with
paraplegia and anemia in March 2013. The medical history of the
patient indicated that a surgical resection of a cardiac
osteosarcoma had been performed at another hospital in September
2008. In May 2010, the patient presented with heart failure and
recurrence of the sarcoma in both atria. Subsequently, the patient
underwent a second surgical resection for the recurrent heart
sarcoma, together with radiotherapy of the heart, and chemotherapy
consisting of adriamycin (ADR), ifsofamide (IFO) and gemcitabine
(GEM), post-operatively. Positron emission tomography-computed
tomography (PET-CT) revealed multiple bone metastases in July 2011,
and therefore radiotherapy to the mandible and scapula, Sr89, and
Pazopanib were added to the treatment regimen. In December 2012,
magnetic resonance imaging revealed metastases in the thoracic
vertebrae, causing paraplegia to develop in March, 2013.
Radiotherapy to the thoracic vertebrae Th4-9 and chemotherapy (ADR,
IFO) were administered to treat the metastases, together with nerve
decompression surgery to the thoracic spinal nerves of the Th4, Th9
vertebrae. Although the paralysis was controlled by these
treatments, the patient was anemic, as indicated by a blood test. A
fecal occult blood test (FOB-test) was performed to determine the
cause of the anemia and the positive results predicted a rectal
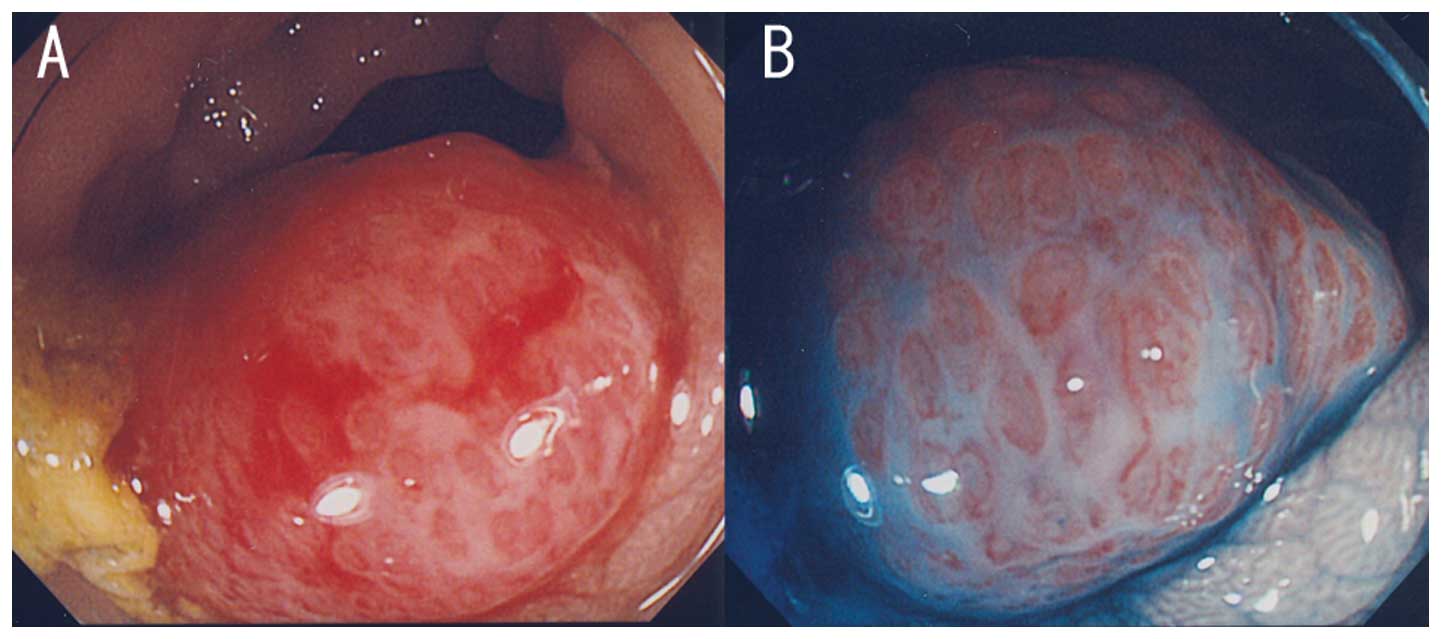
tumor. Colonoscopy revealed a rectosigmoid tumor as the cause of
the bleeding, but this tumor did not have a pit-pattern typical of
rectal cancer (Fig. 1).
Contrast-enhanced computed tomography (CT) showed the tumor in the
rectum with no metastatic lymph nodes (Fig. 2). Additionally, the tumor exhibited
a high fluorodeoxyglucose uptake, similar to other bone metastases,
in PET-CT imaging.
Histological examination of the biopsy sample
revealed growth of spindle cells with irregular nuclei.
Immunohistochemical examination showed positive staining for Ki67
in 5–10% of the cells. These findings were compatible with a
histological diagnosis of a metastatic osteosarcoma. To avoid
bleeding from the tumor and future obstruction of the intestine, a
laparoscopic rectectomy following indocyanine green marking
(12) was performed to completely
remove the rectal tumor (Fig. 3).
Histological examination of this tumor specimen revealed dense
groups of polygonal and spindle cells, with eosinophilic cytoplasms
and pleomorphic nuclei with high density chromatin and irregular
nucleoli. The osteoid matrix did not appear to have any
calcification and there was no lymph node metastasis. These
pathological findings were also detected in the cardiac
osteosarcoma sample (Fig. 4). Thus,
these findings were compatible with a histological diagnosis of a
metastatic rectal osteosarcoma originating from the heart.
The patient recovered without any complications, and
radiotherapy to thoracic vertebrae 12 to lumba vertebrae 5, and
chemotherapy with ADR and cisplatin were administered
post-operatively to treat the bone metastases. The patient was
discharged from the hospital on postoperative day 67 and remained
alive 61 months after the initial operation. The patient is still
receiving chemotherapy and radiotherapy for the bone
metastases.
Discussion
Life-threatening consequences of primary malignant
cardiac tumors include obstruction to the intracardiac blood flow,
interference to valve function, arrhythmias, and pericardial
tamponade resulting from local invasion (5,8,13–17).
Complete surgical resection, whenever possible, is considered the
best treatment option (5–11) since it has been associated with an
improved survival period (17 months after complete surgical
resection, as compared with 6 months without resection) (5). In the majority of cases, the patients
develop a local recurrence and metastases following the initial
surgical resection. Under these conditions, several reports have
shown that effective palliation of local recurrences are possible
and effective (8–11,18,19).
Metastasis at the time of presentation has an impact on the
prognosis; the median survival period of patients with metastases
has been reported to be 5 months, as compared with 15 months, in
patients without metastases (5).
Additional therapies, such as chemotherapy and/or radiotherapy,
improve the prognosis of patients with metastatic diseases and
those with a local recurrence (9).
Reported regions of metastases of the cardiac sarcoma (Fig. 5) (5,7,19)
include the lungs, which are the most common site, in addition to
soft tissue (including the mediastinum), bone, brain, and liver.
The lung, thyroid, brain, intestine, peritoneum, bone, and skin
were previously reported as metastatic regions of cardiac
osteosarcoma, with a median survival time of 9 months (range, 0–67
months) (13–17). The present study, to the best of our
knowledge, reports the first case of a metastasis to the rectum,
which was surgically resected and the patient experienced a
prolonged survival as previously defined.
The patient in this case has been alive for 61
months following the first surgical resection, and 37 months after
the presentation of multiple metastases. This is considered
long-term survival. Upon careful analysis, this study proposes that
repeating the surgical resection is the optimum choice of treatment
as it is necessary to remove the rectal metastasis to prevent
anemia and future obstruction To the best of our knowledge, this is
the first reported case of using laparoscopic resection of a rectal
metastasis. Laparoscopic surgery is minimally invasive and feasible
for this type of metastatic tumor. In the present case, the patient
recovered without any complications and was able to undergo
chemotherapy and radiotherapy shortly after the repeated surgical
resection. The literature on sarcoma metastases to the intestine is
limited and there are no reports on metastases to the rectum
(8). Data from the present case
study suggest that where a FOB-test is positive in the sarcoma
patient, it is necessary to perform a colonoscopy in order that a
metastatic lesion is not overlooked. Adjuvant chemotherapy and
radiotherapy remain controversial treatment options for patients
who have undergone a complete surgical resection, and there is no
established approach for the treatment of patients with metastases
(13–19). In this case, complete resection for
the primary cardiac osteosarcoma was performed, although recurrent
local disease and metastases developed later. The patient underwent
chemotherapy and radiotherapy for the bone metastases and surgical
resection of the rectal metastasis. The patient remains alive after
~5 years since the first operation.
In conclusion, it is suggested that aggressive,
complete surgical resection with radio- and/or chemotherapy is an
effective course of treatment for osteosarcomas. This combination
therapy can provide a palliative choice and leads to an improved
prognosis for patients, even those with metastatic sarcomas.
References
|
1
|
Lam KY, Dickens P and Chan AC: Tumors of
the heart. A 20-year experience with a review of 12,485 consecutive
autopsies. Arch Pathol Lab Med. 117:1027–1031. 1993.
|
|
2
|
Reynen K: Frequency of primary tumors of
the heart. Am J Cardiol. 77:1071996.
|
|
3
|
Rivera-Dávila AD and Rodríguez-Ospina L:
Primary cardiac and pericardial tumors. Bol Asoc Med P R.
100:48–54. 2008.
|
|
4
|
Barreiro M, Renilla A, Jimenez JM, et al:
Primary cardiac tumors: 32 years of experience from a Spanish
tertiary surgical center. Cardiovasc Pathol. 22:424–427. 2013.
|
|
5
|
Simpson L, Kumar SK, Okuno SH, et al:
Malignant primary cardiac tumors: review of a single institution
experience. Cancer. 112:2440–2446. 2008.
|
|
6
|
Putnam JB Jr, Sweeney MS, Colon R, et al:
Primary cardiac sarcomas. Ann Thorac Surg. 51:906–910. 1991.
|
|
7
|
Zhang PJ, Brooks JS, Goldblum JR, et al:
Primary cardiac sarcomas: a clinicopathologic analysis of a series
with follow-up information in 17 patients and emphasis on long-term
survival. Hum Pathol. 39:1385–1395. 2008.
|
|
8
|
Agaimy A, Rösch J, Weyand M and Strecker
T: Primary and metastatic cardiac sarcomas: a 12-year experience at
a German heart center. Int J Clin Exp Pathol. 5:928–938. 2012.
|
|
9
|
Hamidi M, Moody JS, Weigel TL and Kozak
KR: Primary cardiac sarcoma. Ann Thorac Surg. 90:176–181. 2010.
|
|
10
|
Kajihara N, Tanoue Y, Eto M, et al:
Surgical experience of cardiac tumors: early and late results. Surg
Today. 36:602–607. 2006.
|
|
11
|
Bakaeen FG, Jaroszewski DE, Rice DC, et
al: Outcomes after surgical resection of cardiac sarcoma in the
multimodality treatment era. J Thorac Cardiovasc Surg.
137:1454–1460. 2009.
|
|
12
|
Miyoshi N, Ohue M, Noura S, et al:
Surgical usefulness of indocyanine green as an alternative to India
ink for endoscopic marking. Surg Endosc. 23:347–351. 2009.
|
|
13
|
Burke AP and Virmani R: Osteosarcomas of
the heart. Am J Surg Pathol. 15:289–295. 1991.
|
|
14
|
López M, Pinto A, Moreno V, Díaz M and
González Barón M: Primary cardiac osteosarcoma. Clin Transl Oncol.
10:515–516. 2008.
|
|
15
|
Gomez-Rubin MC, Rios JC, Dobarro D, et al:
A recidivant primary cardiac osteosarcoma: the role of bone scans.
Cardiovasc Pathol. 19:55–58. 2010.
|
|
16
|
Karagöz Özen DS, Oztürk MA, Selcukbiricik
F, et al: Primary osteosarcoma of the heart: experience of an
unusual case. Case Rep Oncol. 19:224–228. 2013.
|
|
17
|
Hashimoto W, Hashizume K, Ariyoshi T, et
al: Primary cardiac osteosarcoma with imaging that revealed no
calcification. Gen Thorac Cardiovasc Surg. 59:184–186. 2011.
|
|
18
|
Mayer F, Aebert H, Rudert M, et al:
Primary malignant sarcomas of the heart and great vessels in adult
patients - a single-center experience. Oncologist. 12:1134–1142.
2007.
|
|
19
|
Llombart-Cussac A, Pivot X, Contesso G, et
al: Adjuvant chemotherapy for primary cardiac sarcomas: the IGR
experience. Br J Cancer. 78:1624–1628. 1998.
|