Introduction
Myelolipoma is a rare and benign tumor that is
typically asymptomatic. The tumor most frequently develops in the
adrenal gland, and consists of mature adipose tissue and normal
hematopoietic cells (1).
Extra-adrenal myelolipomas are extremely rare, particularly in the
presacral or perineal space (2).
Intrapulmonary myelolipoma is relatively rare; up to now, only 10
cases of intrapulmonary lesions have been reported worldwide
(3–11). Conservative resection strategies may
be appropriate, as recurrence and malignancy have not been
reported. In the present study, a case of intrapulmonary
myelolipoma is described, and the computed tomography (CT) findings
and potential confounding characteristics that may lead to
incorrect diagnoses are reviewed. Informed consent was obtained
from the patient.
Case report
Patient presentation
A 57-year-old female was admitted to the Nanjing
Medical University Affiliated Nanjing Hospital (Nanjing, Jiangsu,
China), with an intermittent fever of 38.6°C that had been apparent
for 13 days. The patient experienced chills, but no coughing or
expectoration. A chest CT scan performed at a local hospital
revealed the presence of a nodule, bronchiectasis and an infection
in the lower lobe of the right lung. Subsequent to treatment with
3,200,000 IU of patulin and antibiotics every 8 h for 5 days
(orally), the patient underwent a follow-up chest CT scan at the
Nanjing Medical University Affiliated Nanjing Hospital, which
revealed a benign nodule and bronchiectasis in the lower lobe of
the right lung. The tumor was observed in the tributary of the
lower right pulmonary vein, but had not altered in size during the
time between the two CT scans. The results of routine blood work
appeared within normal limits. The patient then underwent a
lobectomy of the lower right lung by thoracoscopy. The histological
analysis of the excised specimen identified a myelolipoma
consisting of mature adipose tissue and hematopoietic cells.
CT procedures
A single-spiral CT scanner (Asteion; Toshiba Medical
Systems, Tokyo, Japan) was used to perform the chest scan, using
the following parameters: Tube voltage, 120 kV; tube current, 140
MA; window width, 1,700 Hounsfield units (HU); window level, -550
HU; and matrix size, 480×480 pixels. The CT slice thickness and
interval were each 10 mm. The CT image was obtained from the apex
to the base of the lung, with the patient at full end-inspiration
and in the supine position.
CT findings
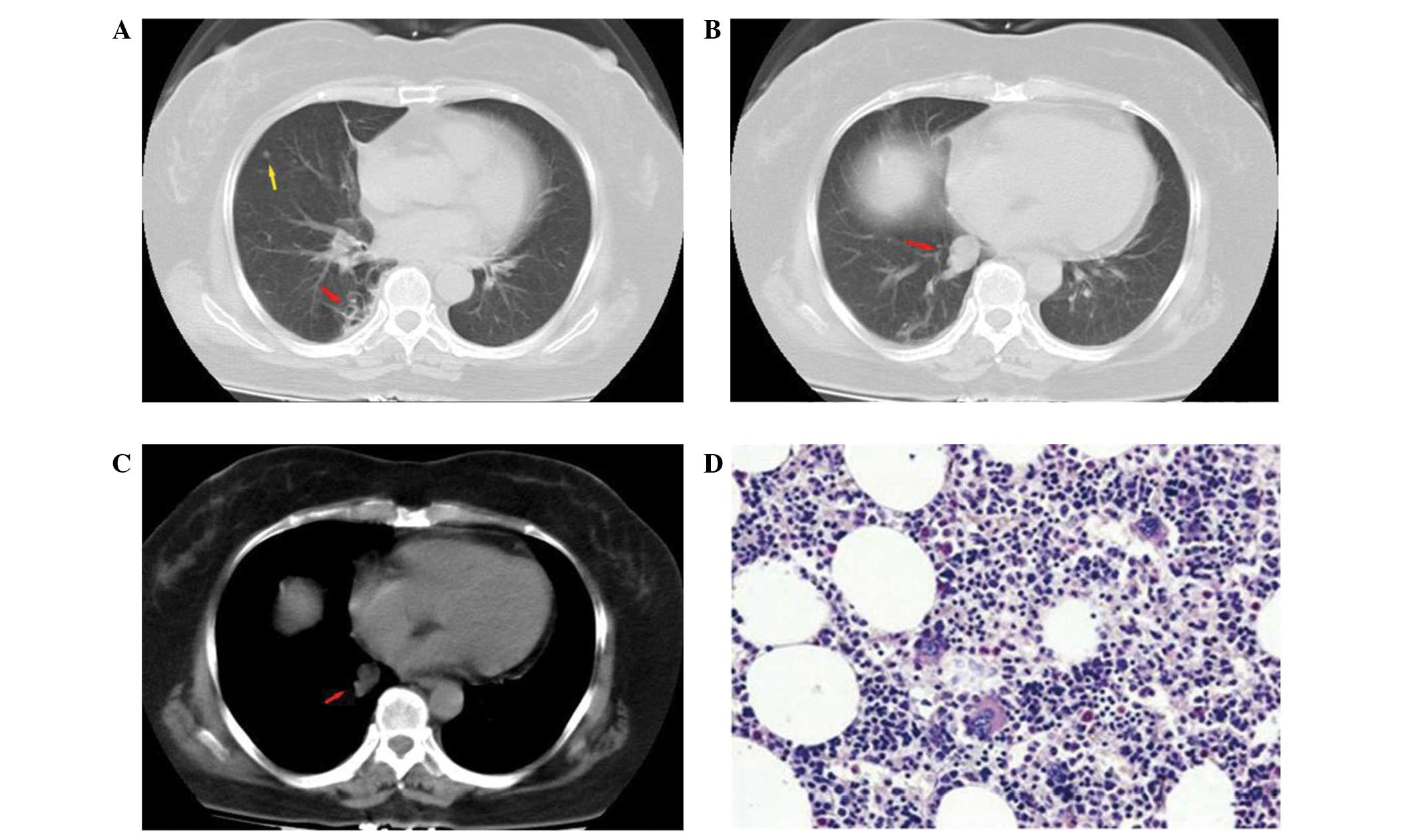
The axial CT images of the chest revealed a smooth
and well-defined nodule of heterogeneous composition in the medial
segment of the lower lobe of the right lung. The largest area of
the nodule in the axial plane was ~14×15 mm. Negative density
values were observed in the mass, with an average density of -46 HU
(range, −30 to −68 HU). The mass was adjacent to the tributary of
the lower right pulmonary vein. No density shadow, indicating
calcification, was detected in the nodule by CT (Fig. 1A and B), and cystic bronchiectasis
was present within the adjacent lung (Fig. 1C).
Pathological findings
Grossly, the nodule was grayish-red and measured 16
mm in diameter at its largest point. Light microscopy revealed that
the tumor was composed of mature adipose tissue and normal mature
hematopoietic cells, including myeloid, erythroid and
megakaryocytic cells, in normal proportions. No trabecular bone,
calcification or ossification was observed in the tumor (Fig. 1D).
Discussion
Myelolipoma was first described in the early 20th
century, and is usually observed in the adrenal gland (1). The occurrence of extra-adrenal
myelolipomas is less common, however, they have been observed in
the presacral soft tissue, retroperitoneum, spleen, liver, stomach,
mediastinum and nasal cavity (2,12–15).
Intrapulmonary myelolipoma is rare, and to the best of our
knowledge, only 10 cases (including three cases reported in the
Chinese literature and the present case) have been documented
(3–11). The patients in these cases ranged in
age between 45 and 81 years, and were predominately male. Table 1 summarizes the patient and tumor
characteristics of the reported intrapulmonary myelolipomas,
including the data from the present study. A diagnosis of
intrapulmonary myelolipoma is usually made when abnormal ratios of
mature adipose tissue and hematopoietic cells, including myeloid,
erythroid and megakaryocytic elements, and occasionally
lymphocytes, are observed histologically (2,4,10,11,15).
 | Table IPatient and tumor characteristics of
reported intrapulmonary myelolipomas. |
Table I
Patient and tumor characteristics of
reported intrapulmonary myelolipomas.
| Case | First author/s
(ref.) | Age,
years/gender | Patient history | Tumor location | Number of sites | Size, cm | Diagnosis method |
|---|
| 1 | Saleeby (11) | 81/F | Pneumonia | Peripherally | Single | ϕ2.5 | Autopsy |
| 2 | Hunter et al
(4) | 70/F | RA, steroid | Peripherally | Multiple | ND | Biopsy |
| 3 | Ziolkowski et
al (9) | 49/M, 59/M | Pneumonia | LLL, RLL | Multiple | 7×5×5, ϕ2 | Autopsy,
resection |
| 4 | Zunarelli et
al (10) | 52/M | MGUS, BC | RLL | Single | ND | Lobectomy |
| 5 | Sabate and Shahian
(7) | 54/M | HC | LUL | Single | ϕ2.5 | Enucleation |
| 6 | Sato et al
(8) | 71/M | Lung cancer | LLL | Single | ϕ2.0 | Autopsy |
| 7 | Lu and Xiao (6) | 45/M | Pneumonia | LUL | Single | ϕ1.5 | Lobectomy |
| 8 | Lin et al
(5) | 45/M | ND | LUL | Single | 4.5×3.5×2.3 | ND |
| 9 | Huang et al
(3) | 53/M | Pneumonia,
atelectasis | LL | Single | 2.3×1.2×1.0 | Biopsy |
| 10 | Present case | 57/F | Bronchiectasis | RLL | Single | ϕ1.6 | Lobectomy |
In total, eight of the 10 previously reported cases
of intrapulmonary myelolipoma were solitary, and two were
multifocal. Intrapulmonary myelolipomas are usually small nodules
measuring <30 mm at their largest dimension, however, one case
revealed a nodule of 7 cm in length (15). Patients with intrapulmonary
myelolipoma usually present with a history of pneumonia, however,
one literature case presented with a bronchial carcinoid tumor
(10), and the patient in the
present study presented with a history of pneumonia and
bronchiectasis. The CT features observed in the present case study
were as expected, with the lesions typically possessing negative HU
values from macroscopic fat. Due to the intermixed hematopoietic
tissue, the attenuation of macroscopic fat is usually heterogeneous
and higher than that of retroperitoneal fat, as was demonstrated in
this patient. Regions of higher density, due to hemorrhage and
calcification, would also be observed. The tumors may also be
mildly or moderately enhanced following administration of
intravenous contrast agents. Upon magnetic resonance imaging,
lesions demonstrate high signal intensity from mature adipose on
T1- and T2-weighted imaging. Fat suppression imaging also reduces
signal intensity in the fatty components of lesions (16). In addition, myeloid elements
demonstrate low signal intensity upon T1-weighted imaging, and
intermediate intensity upon T2-weighted imaging.
CT reveals certain intrapulmonary myelolipomas to be
centrally located masses, leading to obstructive pneumonia and
atelectasis in the lobe or lung segment, and a frequent
misdiagnosis of lung cancer. In these cases, accurate diagnoses are
difficult, even following histological examination of the biopsy
specimens obtained by bronchoscopy (3,6). Upon
CT, negative HU values of adipose components should distinguish
myelolipomas from lung cancer. Intrapulmonary myelolipomas located
in the periphery of the lung, which demonstrate adipose densities
upon CT, are usually small masses with smooth, heterogeneous and
well-defined borders (6). This was
the clinical presentation of the patient in the present study.
Intrapulmonary myelolipomas must be differentiated
from phlebangiomas, hamartomas, lipomas and teratomas.
Intrapulmonary phlebangiomas are rare tumors, which are often
enhanced significantly following administration of intravenous
contrast agents (17). In the
present case study, without CT to identify the lipid component of
the lesion, the nodule in the tributary of the lower-right
pulmonary vein could potentially have been be misdiagnosed as a
phlebangioma. Intrapulmonary hamartomas are common, benign masses
in the pulmonary parenchyma. The histological makeup of these
tumors is characterized by a fibromyxoid stroma, cartilage,
bronchial cells, adipose tissue and bone. The characteristic
‘popcorn-like’ calcification that occurs with these masses is
frequently observed by CT (18).
Intrapulmonary lipomas are exceptionally rare. Only 10 cases have
been reported to date in Medline, and no marked gender differences
are evident with respect to these tumors (19,20).
Pathologically, intrapulmonary lipomas are grossly observed as
being well-defined, thinly-encapsulated and rounded, pale-yellow
masses, which are composed of mature adipose tissue upon
microscopic analysis (19). A
homogeneous and defined lesion that contains a high density of
lipid can be revealed by CT imaging. No contrast enhancement is
observed with these masses, as they lack soft tissues (19,20).
Myelolipomas that are predominantly composed of fatty tissue are
difficult to distinguish from lipomas. Intrapulmonary teratomas may
be malignant and upon histopathology, contain tissue that
originates from any of the three germinal layers. Calcification is
a typical radiological finding and is extremely valuable for
clinical diagnoses when CT reveals discrete areas of soft tissue,
fat, fluid or punctate calcification (20). In the case that peripheral
myelolipomas in the lung are mainly composed of hematopoietic
cells, it may be necessary to perform a percutaneous needle biopsy
for a definite diagnosis.
In general, accurate identification of
intrapulmonary myelolipoma depends on histopathology. However, it
is important to understand the radiological characteristics, which
can provide valuable diagnostic clues in clinical practice.
Although it is difficult to achieve an accurate diagnosis, a chest
CT scan demonstrating a well circumscribed nodule with low
attenuation of adipose tissue is helpful in the diagnosis of
intrapulmonary myelolipomas. Conservative resection strategies may
be appropriate, as recurrence and malignancy have not been
reported. However, given the likelihood of subsequent hemorrhage or
compression of adjacent bronchi by myelolipomas, surgical removal
is the ideal choice.
Acknowledgements
The authors would like to thank Professor Wenbin
Huang, Department of Pathology, Nanjing Medical University
Affiliated Nanjing Hospital (Nanjing First Hospital) for providing
assistance with the pathological analysis.
References
|
1
|
Osborn M, Smith M, Senbanjo T, et al:
Adrenal myelolipoma - clinical, radiological and cytological
findings: a case report. Cytopathology. 13:242–246. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Beiko D, Roldan H, Sengupta SK and George
RL: Laparoscopic excision of a large extra-adrenal perirenal
myelolipoma. Can Urol Assoc J. 4:E39–E41. 2010.PubMed/NCBI
|
|
3
|
Huang WT, Zhao SJ and Lin DM:
Pulmonary-bronchus myelolipoma and review on extra-adrenal
myelolipomas in Chinese literature. Chin Med J (Engl).
125:3188–3190. 2012.
|
|
4
|
Hunter SB, Schemankewitz EH, Patterson C
and Varma VA: Extraadrenal myelolipoma. A report of two cases. Am J
Clin Pathol. 97:402–404. 1992.PubMed/NCBI
|
|
5
|
Lin XY, Song YH and Wang JY: Cystic lung
myelolipoma with bone and cartilage metaplasia: A
clinicopathological observation. J Diag Pathol. 16:55–57. 2009.
|
|
6
|
Lu X and Xiao L: Myelolipoma of the lung:
a case report. Chin Med J (Engl). 116:951–953. 2003.
|
|
7
|
Sabate CJ and Shahian DM: Pulmonary
myelolipoma. Ann Thorac Surg. 74:573–575. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Sato K, Ueda Y, Katsuda S and Tsuchihara
K: Myelolipoma of the lung: a case report and brief review. J Clin
Pathol. 60:728–730. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Ziókowski P, Muszczyńska-Bernhard B and
Dziegiel P: Myelolipoma: the report of two cases in pulmonary
location. Pol J Pathol. 47:141–142. 1996.
|
|
10
|
Zunarelli E, Criscuolo M, Malavolta L,
Piccinini L and Barbolini G: A case of lung myelolipomatosis in a
patient with bronchial carcinoid. Panminerva Med. 41:175–178.
1999.PubMed/NCBI
|
|
11
|
Saleeby ER: Heterotopia of the bone marrow
without apparent cause. Am J Pathol. 1:69–76.3. 1925.PubMed/NCBI
|
|
12
|
Arpino L, Capuano C and Franco A:
Intradural thoracic myolipoma. ANZ J Surg. 81:8432011. View Article : Google Scholar
|
|
13
|
George SA, Manipadam MT and Thomas R:
Primary myelolipoma presenting as a nasal cavity polyp: a case
report and review of the literature. J Med Case Rep. 6:1272012.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Radhi J: Hepatic myelolipoma. J
Gastrointestin Liver Dis. 19:106–107. 2010.PubMed/NCBI
|
|
15
|
Vaziri M, Sadeghipour A, Pazooki A and
Shoolami LZ: Primary mediastinal myelolipoma. Ann Thorac Surg.
85:1805–1806. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Guo YK, Yang ZG, Li Y, et al: Uncommon
adrenal masses: CT and MRI features with histopathologic
correlation. Eur J Radiol. 62:359–370. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Mao Q, Xiang ST, Bao YM, et al: Pulmonary
phlebangiomas under the upper ulmonary vein: A case report. Chin J
Radiol. 38:10062004.(In Chinese).
|
|
18
|
Madan K, Sharma S, Singh N and Radhika S:
Large pulmonary hamartoma with ‘popcorn’ like calcification.
Monaldi Arch Chest Dis. 75:243–244. 2011.
|
|
19
|
Moran AM, Jian B, Min H, Pechet T and Fogt
F: Peripheral intrapulmonary lipoma in a 26-year-old woman - a case
report. Pol J Pathol. 62:113–115. 2011.PubMed/NCBI
|
|
20
|
Rana SS, Swami N, Mehta S, Singh J and
Biswal S: Intrapulmonary teratoma: an exceptional disease. Ann
Thorac Surg. 83:1194–1196. 2007. View Article : Google Scholar : PubMed/NCBI
|