Introduction
Lung adenocarcinoma is one of the main causes of
cancer-related mortality globally, accounting for nearly 30% of
cancer-related mortalities worldwide (1). The incidence of lung adenocarcinoma is
rising all over the world due to the adoption of lifestyle choices
that have an association with cancer, including physical inactivity
and smoking. Although advances have been made with regard to early
diagnosis and treatment modalities, the prognosis for affected
patients remains poor, with a five-year survival rate of only ~15%
(2). As a consequence, the prevention
of lung cancer is a high priority and urgent efforts are required
to identify measures, including drug treatment, which may
effectively reduce the risk of lung cancer. Chemotherapy is one of
the best approaches for unresectable tumors, but the efficacy of
current lung tumor chemotherapy is only modest and the requirement
for an optimal lung adenocarcinoma treatment remains. Metformin, a
biguanide drug, has been demonstrated to exert anticancer effects
(3). The drug reduces the level of
glucose by decreasing liver glucose production, thereby increasing
fatty acid oxidation and glucose utilization. Notably, previous
epidemiological studies suggested that patients with diabetes who
were treated with metformin had a lower cancer-related mortality
rate and a lower incidence rate of cancer of any type when compared
with patients who underwent other treatments (4–7).
Additionally, metformin was shown to prevent the induction of
carcinogen-induced pancreatic cancer in hamsters that were
maintained on high-fat diets (8). The
drug was also shown to inhibit the growth of breast and colon
carcinoma cells (9,10). Collated evidence from a number of
clinical studies has recently been published in a meta-analysis
(11). However, the precise
mechanisms involved remain incompletely understood. The antitumor
activity of metformin may be explained by two mechanisms. Firstly,
metformin is able to decrease insulin resistance and lower the
levels of circulating insulin by activating AMP-activated protein
kinase (AMPK), which causes decreased hepatic gluconeogenesis
(10) and increased glucose uptake in
the muscle. Secondly, metformin acts as an inhibitor of tumor
growth, at least in part by upregulating the activity of AMPK and
by downstream suppression of signaling through the mammalian target
of rapamycin (mTOR) (12). Several
other potential mechanisms for the anticancer action of metformin
have also been demonstrated, including the suppression of HER2
oncoprotein expression, the downregulation of cyclin D1 expression
and p53 activation (9,13–15).
However, there have been few studies evaluating the potential
utility of metformin in in vivo models of cancer, and the
method by which metformin induces apoptosis remains unknown. The
present study describes experiments that were performed to
investigate the hypothesis that metformin exhibits direct
anti-proliferative actions on lung adenocarcinoma cells in
vitro and in vivo.
Materials and methods
Chemicals and reagents
Metformin was obtained from Sigma-Aldrich (St.
Louis, MO, USA) and dissolved in phosphate-buffered saline (PBS).
Cell culture chemicals and materials were obtained from Invitrogen
Life Technologies (Burlington, ON, Canada). Anti-β-actin,
anti-B-cell lymphoma (Bcl)-2, anti-Bax and anti-caspase-3 were
purchased from Cell Signaling Technology (Beverly, MA, USA).
Horseradish peroxidase-conjugated anti-rabbit immnoglobulin (Ig)G,
anti-mouse IgG and enhanced chemiluminescence (ECL) reagents were
obtained from Amersham Pharmacia Biotech (Piscataway, NJ, USA).
Cell lines and culture conditions
The human lung adenocarcinoma A549 cells were
obtained from the Shanghai Institute of Cell Biology, Chinese
Academy of Sciences (Shanghai, China). The A549 cells were
maintained in Dulbecco's modified Eagle's medium (DMEM)
supplemented with 10% fetal bovine serum, 2 mmol/l L-glutamine, 100
U/ml penicillin and 100 µg/ml streptomycin at 37°C, in an
atmosphere of 5% CO2. The cells were passaged by 0.25%
Trypsin-EDTA when they reached 80% confluence.
Cell proliferation assay
An MTT assay was used to evaluate the effect of
metformin on the lung adenocarcinoma cells. Briefly, ~10,000 cells
were seeded into 96-well tissue culture plates and then treated
with different doses (0, 5, 10, 20 and 50 mmol/l) of metformin for
24, 48 and 72 h, respectively. MTT reagent was then added to each
well, and the cells were further incubated for 6 h. Absorbance was
measured in an automated microplate reader (ELX 800; BioTek
Instruments, Inc., Winooski, VT, USA) at 450 nm.
Cell morphological analysis
The A549 cells were treated with 10.0 mM metformin
or 0.1% dimethyl sulfoxide (control) for 48 h. The cells were then
incubated with 10 µg/ml Hoechst 33342 and observed by fluorescence
microscope (DMIRB; Leica, Wetzler, Germany).
Flow cytometry
The A549 cells were starved of serum for 24 h and
then treated with different doses (0, 10 and 20 mmol/l) of
metformin for 48 h. The cells were then washed with PBS (pH 7.4)
and fixed with 70% ice-cold ethanol at 4°C overnight. After
fixation, the cells were stained with propidium iodide (PI) at 1
mg/ml for 30 min at room temperature. The cell cycle was analyzed
by flow cytometry (FACScan; BD Biosciences, Franklin Lakes, NJ,
USA).
For cell apoptosis detection, the apoptotic rate of
A549 cells was analyzed using an Annexin V-fluorescein
isothiocyanate (FITC) apoptosis detection kit (Nanjing KeyGen
Biotech Co., Ltd., Nanjing, China). A total of 1×105
cells/well were seeded into six-well plates and cultured in DMEM at
37°C overnight. Subsequent to starvation for 12 h, the cells were
treated with different doses of metformin (0, 10 and 20 mmol/l) in
complete medium for 48 h, digested with 2.5 mg/ml trypsin, washed
twice with PBS and suspended with 300 µl binding buffer (Nanjing
KeyGen Biotech Co., Ltd.). The cells were then incubated with 2 µl
Annexin V and 5 µl PI for 15 min at room temperature, and the
distribution of viable, early apoptotic, late apoptotic and
necrotic cells was detected using a FACSCaliber flow cytometer (BD
Biosciences). Cells that were negative for the Annexin V-FITC and
PI were considered to be viable cells, cells that were positive for
Annexin V-FITC, but negative for PI were considered to be early
apoptotic cells, cells that were positive for Annexin V-FITC and PI
were considered to be late apoptotic cells, while cells that were
negative for both Annexin V-FITC and PI were considered to be
necrotic. The sum of the early and late apoptotic cells constituted
the total number of apoptotic cells, which was presented as the
percentage of the total cells.
Mitochondrial and cytosolic
fractionation
The Cell Mitochondria Isolation kit (Beyotime
Institute of Biotechnology, Haimen, China) was used to perform the
isolation of the mitochondria and cytosol, according to the
manufacturer's instructions. Samples of cytosol and mitochondria
were dissolved in lysis buffer, and proteins were subjected to
western blotting, respectively.
Western blot analysis
The A549 cells were lysed in a
radioimmunoprecipitation assay buffer (9.1 mM dibasic sodium
phosphate, 1.7 mM monobasic sodium phosphate, 150 mM NaCl, 1% NP40,
0.5% sodium deoxycholate, 0.1% SDS, 0.2 mM sodium vanadate, 0.2 mM
phenylmethylsulfonyl fluoride and 0.2 U/ml aprotinin). Clarified
protein lysates (50 g) were resolved electrophoretically on
denaturing SDS-polyacrylamide gels (10%), and transferred to
nitrocellulose membranes. The membranes were then blocked with 1%
bovine serum albumin at room temperature for 1 h and then incubated
with the indicated specific primary antibodies for 3 h. Proteins
were visualized with Horseradish peroxidase (HRP)-conjugated
secondary antibodies. To corroborate equal loading, membranes were
stripped and reprobed using an antibody specific for β-actin.
Finally, antigen-antibody complexes were detected using the ECL
system.
A549 tumor xenograft
A total of 6×106 A549 cells were injected
into the right flank of 30 BALB/c nude mice (supplied by the
Experimental Animal Department of Binzhou medical College,
Shandong, China). Seven days later, 25 mice with tumors ~100
mm3 in size were randomly distributed into the following
five groups: Control group (PBS), low-dose metformin (40 mg/kg/day)
group, high-dose metformin (200 mg/kg/day) group, cisplatin (5
mg/kg/day) group and metformin (40 mg/kg/day) plus cisplatin (5
mg/kg/day) group. Tumor volume (mean values and 95% confidence
intervals) was measured every three days after the initial
injection. After 18 days, the mice were sacrificed by cervical
dislocation and the tumor weights were measured. The study was
approved by the ethics committee of Binzhou Medical College
(Binzhou, China).
Statistical analysis
All experiments, except that of the nude mice study,
were repeated at least three times and the values are expressed as
the mean ± standard deviation. Statistical significance was
determined by Student's t-test. P<0.05 was considered to
indicate a statistically significant difference.
Results
Metformin inhibits human lung
carcinoma A549 survival in a dose- and time-dependent manner
The viabilities of A549 cells treated with different
concentrations of metformin (0, 5, 10, 20 and 50 mmol/l) for
different time periods (0, 24, 48 and 72 h) were determined using
MTT assay. As shown in Fig. 1A, the
cell viabilities were decreased in a dose- and time-dependent
manner. Cisplatin is the most active treatment for lung carcinoma,
however, the sensitivity of tumor cells to cisplatin varies. The
present results indicated that metformin could increase the
cytotoxicity of cisplatin in A549 cells (Fig. 1B).
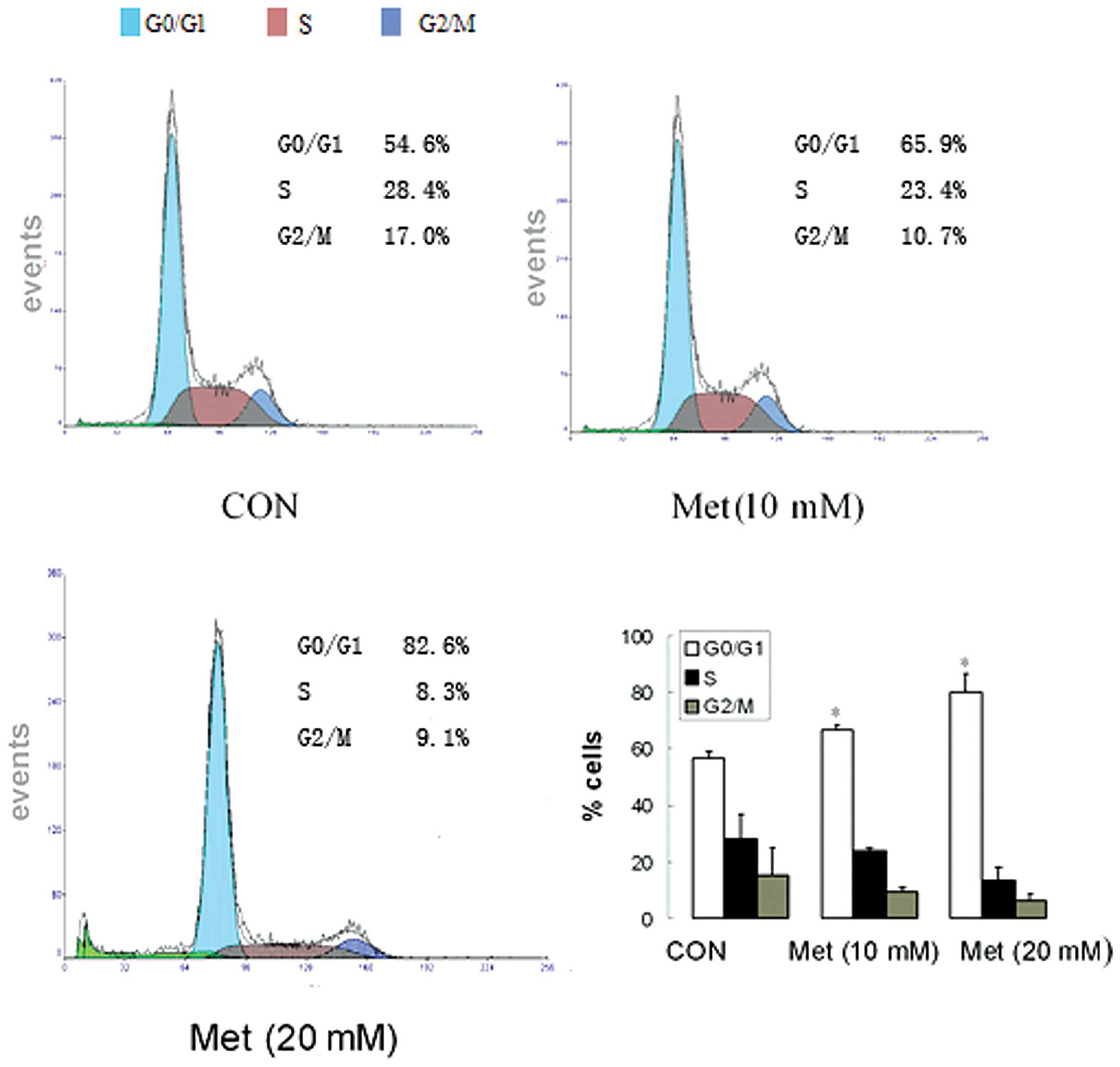
Metformin induces cell cycle arrest in
the G0/G1 phase in human lung adenocarcinoma
cells
To identify the effect of metformin on the cell
cycle of human lung carcinoma cells, the cell cycle distribution of
A549 cells treated with different concentrations of metformin (0,
10 and 20 mmol/l) for 48 h was determined using a PI staining
assay. As shown in Fig. 2, metformin
induced cell cycle arrest in the G0/G1 phase
in the A549 cells. Treatment with different doses of metformin (10
or 20 mM) for 48 h resulted in an increase in A549 cells in the
G0/G1 population, to 65.9 and 82.6%,
respectively, compared with 54.6% in the untreated control group
(Fig. 2).
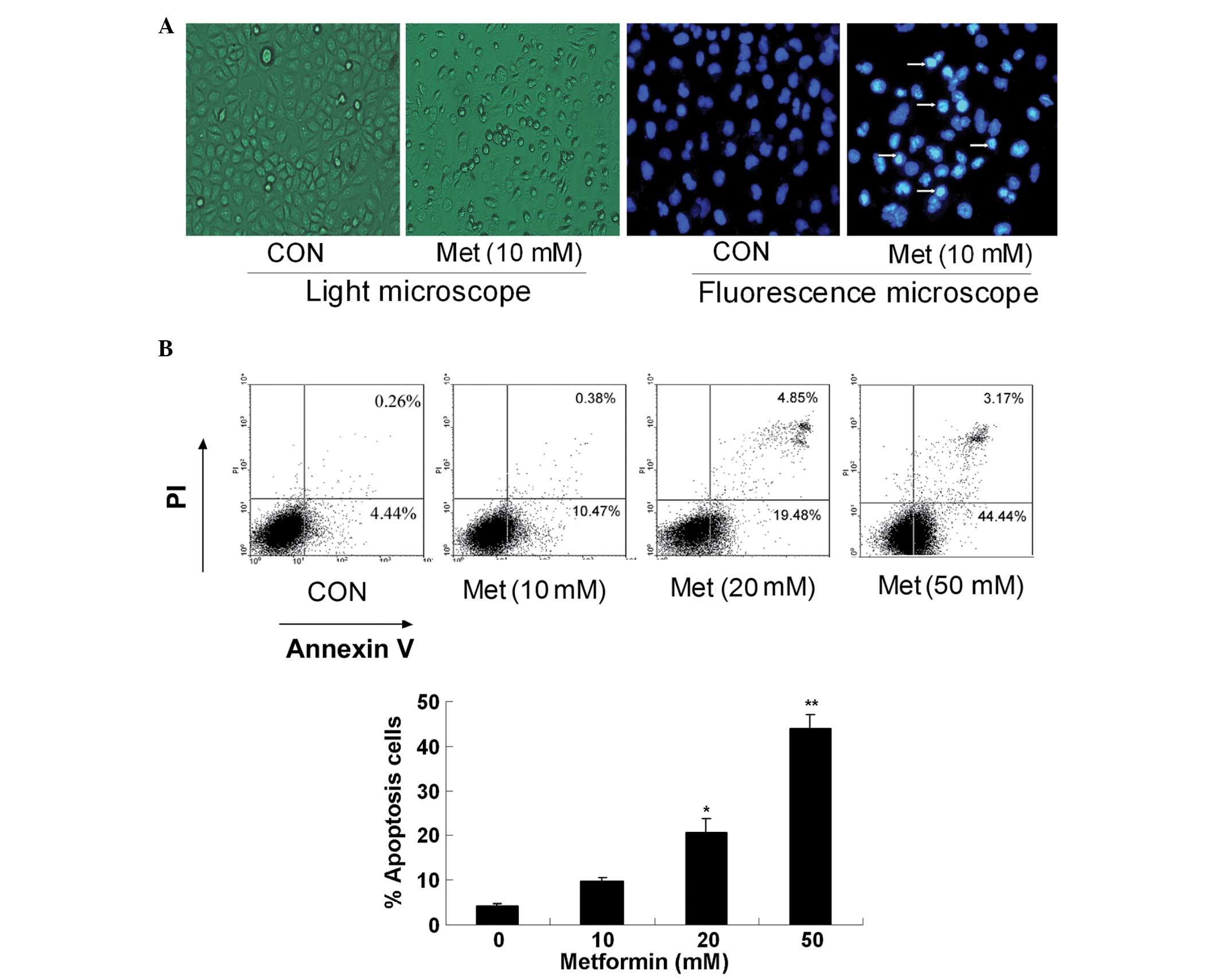
Metformin induces apoptosis in human
lung adenocarcinoma cells
Hoechst-33342 and Annexin-V/PI staining assays were
combined to investigate whether metformin can induce A549 cell
apoptosis. First, the apoptotic morphology of the A549 cells
treated with 10.0 mM metformin for 24 h was observed, and the
metformin-treated cells were shown to manifest brighter, granular,
blue fluorescence and more apoptotic bodies compared with control
group (Fig. 3A). The percentage of
apoptotic cells was determined by cell flow cytometric analysis
following PI staining. Compared with the untreated cells, the cells
treated with metformin for 48 h underwent apoptosis in a
dose-dependent manner (Fig. 3B).
Metformin induces apoptosis mainly
through the mitochondria-mediated pathway
The treatment with metformin decreased the
expression of Bcl-2 and Bcl-extra large (Bcl-xl), and increased the
expression of Bax in a dose-dependent manner in the A549 cells, as
determined by western blot analysis (Fig.
4A). Downstream of the apoptosis signaling pathways, there is
significant cleavage activation of caspase-3 and poly(ADP-ribose)
polymerase (PARP) (Fig. 4B). A
significant release of cytochrome c from the mitochondria to
the cytosol was observed after the cells were treated with
metformin (Fig. 4C). These results
indicate that metformin induces apoptosis mainly through the
mitochondria-mediated internal pathway in lung carcinoma cells.
Metformin suppresses tumor
proliferation in vivo
In order to determine whether metformin could affect
tumor growth, the effect of metformin on tumor growth inhibition
was studied in vivo via intraperitoneal injection. It was
found that tumor growth was markedly inhibited in the high-dose
metformin and metformin plus cisplatin groups (Fig. 5A). Compared with the control group,
the tumor xenograft treated with metformin (200 mg/kg/day) was
signifiantly decreased in size (Fig.
5B). In addition, there was a signifiant decrease in tumor size
in the metformin (40 mg/kg/day) plus cisplatin group, when compared
with the other groups (Fig. 5C). The
tumor volume of the high-dose metformin and metformin plus
cisplatin groups was 611.4±51.5 and 281.6±21.1 mm3,
respectively, compared with the control group (1,042.4±39.7
mm3). The tumor growth inhibition rate was 41.3% in the
high-dose metformin group (P<0.01) and 72.9% in the metformin
plus cisplatin group (P<0.01) compared with the control
(Fig. 5D). Body weight reduction is
an indicator of drug toxicity. In the high-dose metformin and
metformin plus cisplatin groups, body weight was 22.31±1.69 and
23.83±2.39 g, respectively (Fig. 5E),
which was comparable to the control group.
Discussion
Metformin has a long history of human use, with less
toxicity and a relatively low cost when compared with other
antidiabetic drugs. The drug is now widely used as a first-line
treatment for type II diabetes (16).
Notably, numerous studies have indicated that metformin could
protect patients with type II diabetes from cancer and inhibit
cancer cell proliferation in vitro (17–22).
According to the present study, metformin is a potent inhibitor of
cell proliferation in the A549 cell line. For example, inhibition
of cell proliferation was observed in the A549 cells treated with
20 mM metformin for 48 h, with a 63% decrease in cell viability.
The study then analyzed whether metformin affects the cell cycle.
To determine this, proliferating A549 cells were treated with
metformin for 48 h at different concentrations. As shown in
Fig. 2, an increasing number of cells
accumulated in the G0/G1 phase. In parallel,
a reduced percentage of cells was observed in the S and
G2/M phases. In order to determine whether metformin
induces apoptosis in A549 cells, an Annexin V-fluorescein
isothiocyanate labeling assay and found that metformin at
concentrations of <5 mM did not affect the amount of Annexin
V-positive cells (data not shown). However, metformin at a
concentration of >5 mM increased the percentage of cells
positive for Annexin V. These results indicate that metformin can
induce apoptosis, but only at high concentrations.
There are two classic apoptotic pathways in
mammalian cells, namely the mitochondria-mediated apoptotic pathway
and the death receptor-mediated apoptotic pathway, and there is
cross-talk between the two. To further clarify the apoptotic
molecular mechanisms of human lung carcinoma cells induced by
metformin, the total proteins of the A549 cells treated with
different concentrations of metformin for 24 h were analyzed using
a western blot assay. Using the present data, it may be concluded
that metformin induces the apoptosis of A549 cells in vitro
mainly via the mitochondria-mediated internal pathway, which is
initiated by a range of apoptosis-inducing signals that cause an
imbalance in the major apoptosis regulators, the proteins of the
Bcl-2 family, such as Bcl-2, Bcl-xl and Bax. Bax, a pro-apoptotic
protein, accumulates on the mitochondria subsequent to being
activated, and triggers the permeability of the outer mitochondrial
membrane to increase. As a result, the mitochondria release
cytochrome c. This, in turn, activates downstream death
programs, such as caspase 3 and PARP. These observations suggested
that modulation of the mitochondria-mediated pathway may be an
important mechanism underlying the biological effects of metformin.
The present study results are similar to those in the study by
Gotlieb et al (23), which
reported that metformin significantly inhibits the ovarian cancer
cell line growth and potentiates the effects of cisplatin.
Additionally, the inhibition of growth by metformin was partially
abolished by the AMPK inhibitor, compound C. The study also
discovered that metformin-induced anti-proliferation is associated
with the phosphorylation of AMPK and the decrease of p-p70S6K
(23). Another study found that
metformin was able to induce apoptosis in vitro in colon
cancer cells, but only in those cells that were p53-deficient
(9). A subsequent study found that
metformin in combination with paclitaxel resulted in mainly
G2 arrest and decreased human telomerase reverse
transcriptase mRNA expression. Metformin was demonstrated to
potentiate the effects of paclitaxel in endometrial cancer cells by
inhibiting cell proliferation and modulating the mTOR pathway
(24). In another study, metformin
was found to decrease high-fat-induced cardiac cell death by
inhibiting ceramide synthesis. However, proton and lactate
accumulation are induced by metformin, which leads to
caspase-3-independent cell damage at high concentrations (25). These studies indicate that metformin
mediates its effects through a range of mechanisms.
In vivo, the present data showed that the
high-dose metformin and metformin plus cisplatin groups could
significantly decrease A549 tumor growth without any significant
side-effects, including weight loss, hair loss, dysphoria or
lethargy. The present results are of particular significance since
this is the first time that metformin has been shown to inhibit
lung adenocarcinoma growth in a xenograft model. Similar to the
present study, a study by Huang et al reported that
metformin delayed the onset of tumors, but in mice deficient in the
phosphatase and tensin homolog tumor suppressor (26). Ben Sahra et al found that
metformin inhibited prostatic tumor growth in vivo (27). Another study also found that metformin
could prevent pancreatic cancer in hamsters fed a high-fat diet and
exposed to pancreatic carcinoma (8).
Thus, in summary, the present study is a preliminary
study suggesting that metformin selectively induces the apoptosis
of lung carcinoma A549 cells via the mitochondria-mediated internal
pathway. Although metformin has been demonstrated to inhibit
proliferation in vitro in prostate, breast, colon and
ovarian cancer cell lines, the present study observed its effect on
lung adenocarcinoma for the first time. The results support the
development of pre-clinical experiments to further evaluate the
potential role of combining metformin with chemotherapy as a new
treatment for lung adenocarcinoma. Further long-term studies of
metformin are required in patient populations of similar and larger
sizes in order to confirm these observations.
Acknowledgements
This study was supported by a grant from the
National Science and Technology Special Foundation for Major
Infectious Diseases Prevention and Control (No. 2008Ex
10002019).
References
|
1
|
Jemal A, Siegel R, Xu J and Ward E: Cancer
statistics, 2010. CA Cancer J Clin. 60:277–300. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Mulshine JL and Sullivan DC: Clinical
practice. Lung cancer screening. N Engl J Med. 352:2714–2720. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Dowling RJ, Goodwin PJ and Stambolic V:
Understanding the benefit of metformin use in cancer treatment. BMC
Med. 9:332011. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Evans JM, Donnelly LA, Emslie-Smith AM, et
al: Metformin and reduced risk of cancer in diabetic patients. BMJ.
330:1304–1305. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Bowker SL, Majumdar SR, Veugelers P and
Johnson JA: Increased cancer-related mortality for patients with
type 2 diabetes who use sulfonylureas or insulin. Diabetes Care.
29:254–258. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Lee MS, Hsu CC, Wahlqvist ML, et al: Type
2 diabetes increases and metformin reduces total, colorectal, liver
and pancreatic cancer incidences in Taiwanese: a representative
population prospective cohort study of 800,000 individuals. BMC
Cancer. 11:202011. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Zhu Z, Jiang W, Thompson MD, et al:
Metformin as an energy restriction mimetic agent for breast cancer
prevention. J Carcinog. 10:172011. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Schneider MB, Matsuzaki H, Haorah J, et
al: Prevention of pancreatic cancer induction in hamsters by
metformin. Gastroenterology. 120:1263–1270. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Buzzai M, Jones RG, Amaravadi RK, et al:
Systemic treatment with the antidiabetic drug metformin selectively
impairs p53-deficient tumor cell growth. Cancer Res. 67:6745–6752.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Dowling RJ, Zakikhani M, Fantus IG, et al:
Metformin inhibits mammalian target of rapamycin dependent
translation initiation in breast cancer cells. Cancer Res.
67:10804–10812. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Noto H, Goto A, Tsujimoto T and Noda M:
Cancer risk in diabetic patients treated with metformin: a
systematic review and meta-analysis. PLoS One. 7:e334112012.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Shaw RJ, Lamia KA, Vasquez D, et al: The
kinase LKB1 mediates glucose homeostasis in liver and therapeutic
effects of metformin. Science. 310:1642–1646. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Ben Sahra I, Laurent K, Loubat A, et al:
The antidiabetic drug metformin exerts an antitumoral effect in
vitro and in vivo through a decrease of cyclin D1 level. Oncogene.
27:3576–3586. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Zhuang Y and Miskimins WK: Cell cycle
arrest in Metformin treated breast cancer cells involves activation
of AMPK, downregulation of cyclin D1 and requires p27Kip1 or
p21Cip1. J Mol Signal. 3:182008. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Vazquez-Martin A, Oliveras-Ferraros C and
Menendez JA: The antidiabetic drug metformin suppresses HER2
(erbB-2)oncoprotein overexpression via inhibition of the mTOR
effector p70S6K1 in human breast carcinoma cells. Cell Cycle.
8:88–96. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Bailey CJ and Turner RC: Metformin. N Engl
J Med. 334:574–579. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Wang LW, Li ZS, Zou DW, et al: Metformin
induces apoptosis of pancreatic cancer cells. World J
Gastroenterol. 14:7192–7198. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Hirsch HA, Iliopoulos D, Tsichlis PN and
Struhl K: Metformin selectively targets cancer stem cells and acts
together with chemotherapy to block tumor growth and prolong
remission. Cancer Res. 69:7507–7511. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Cantrell LA, Zhou C, Mendivil A, et al:
Metformin is a potent inhibitor of endometrial cancer cell
proliferation - implications for a novel treatment strategy.
Gynecol Oncol. 116:92–98. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Goodwin PJ, Stambolic V, Lemieux J, et al:
Evaluation of metformin in early breast cancer: a modification of
the traditional paradigm for clinical testing of anti-cancer
agents. Breast Cancer Res Treat. 126:215–220. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Xiong Y, Lu QJ, Zhao J and Wu GY:
Metformin inhibits growth of hepatocellular carcinoma cells by
inducing apoptosis via mitochondrion-mediated pathway. Asian
Pacific J Cancer Prev. 13:3275–3279. 2012. View Article : Google Scholar
|
|
22
|
Soranna D, Scotti L and Zambon A: Cancer
risk associated with use of metformin and sulfonylurea in type 2
diabetes: a meta-analysis. Oncologist. 17:813–822. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Gotlieb WH, Saumet J, Beauchamp MC, et al:
In vitro metformin anti-neoplastic activity in epithelial ovarian
cancer. Gynecol Oncol. 110:246–250. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Hanna RK, Zhou C, Malloy KM, et al:
Metformin potentiates the effects of paclitaxel in endometrial
cancer cells through inhibition of cell proliferation and
modulation of the mTOR pathway. Gynecol Oncol. 125:458–469. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
An D, Kewalramani G, Chan JK, et al:
Metformin influences cardiomyocyte cell death by pathways that are
dependent and independent of caspase-3. Diabetologia. 49:2174–2184.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Huang X, Wullschleger S, Shpiro N, et al:
Important role of the LKB1-AMPK pathway in suppressing
tumorigenesis in PTEN-deficient mice. Biochem J. 412:211–221. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Ben Sahra I, Laurent K, Loubat A, et al:
The antidiabetic drug metformin exerts an antitumoral effect in
vitro and in vivo through a decrease of cyclin D1 level. Oncogene.
27:3576–3586. 2008. View Article : Google Scholar : PubMed/NCBI
|