Introduction
Iron deficiency anemia (IDA) is reported to occur in
2–5% of men and postmenopausal women in the developed world
(1). Complete endoscopic
investigation is recommended, since gastrointestinal cancer occurs
in 10–20% of IDA patients (2–7). Despite this recommendation, only 30–50%
of patients who are diagnosed with IDA receive an endoscopic
examination within 4 months (8,9). This
cannot be explained as the patient's unwillingness for treatment,
as it is common in daily practice for patients undergoing treatment
for IDA to have received no investigation for the potential cause
(10). Based on this data,
interventions besides the aforementioned recommendation are
required for a change in daily practice (8). The importance of IDA must be recognized,
as IDA-associated diagnostic testing is one of the most
underutilized diagnostic opportunities in colorectal cancer
(11). Although the importance of IDA
examination is emphasized as an opportunity to identify
gastrointestinal cancer, there are only a small number of reports
regarding the staging and resectability of gastrointestinal cancer
identified through diagnosis of IDA (12).
Japan has a national health insurance system that
promotes annual medical check-ups, and is one of the very few
countries with a medical system that is prepared for daily
endoscopic examinations in municipal hospitals and clinics. Data on
endoscopy has been accumulated by hospitals in Japan; however,
there are no studies about the staging and resectability of
gastrointestinal cancer cases that are identified during the
examination of patients with IDA in Japan. The present study was
conducted to profile the gastrointestinal cancer cases identified
during examination of IDA patients, in order to re-emphasize the
importance of IDA examination and confirm the rate of
gastrointestinal cancer detection from the examination of IDA
patients in a municipal hospital in Japan.
Patients and methods
Inclusion criteria
Patients (including females >51 and males >18
years old) who were diagnosed with IDA at the internal medicine
outpatient clinic of Asahi General Hospital (Chiba, Japan) between
1 April 2010 and 31 March 2012 were included in the retrospective
study. Data of these 472 patients were extracted and analyzed.
Excel 2013 (Microsoft Corporation, Redmond, WA, USA) was used to
calculate means and standard deviation for the data. The diagnosis
of IDA was made based on hemoglobin levels <135 g/l for men, and
<120 g/l for women, combined with a serum ferritin level of
<33.71 pmol/l (15 ng/ml) (13,14). IDA
patient data and details of examinations were selected from
electronic patient records, and information regarding staging,
treatment and clinical course were extracted for each patient
diagnosed with cancer.
Exclusion criteria
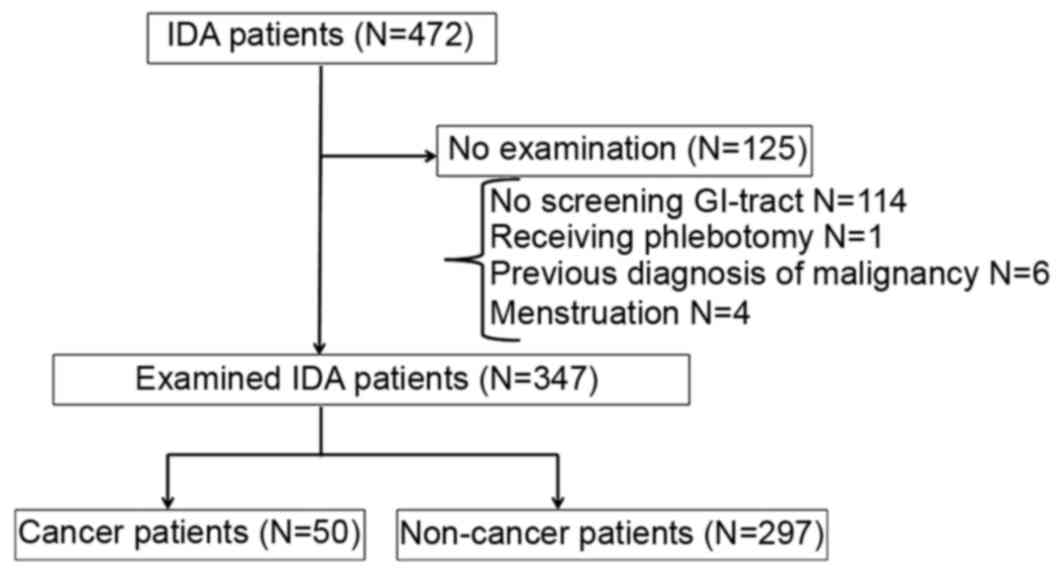
The exclusion criteria were as follows: Patients who
had not received any investigation for gastroscopy or colonoscopy;
females who were still undergoing menstruation; patients who had a
previous diagnosis for malignancy including recurrence; and
patients who had recently undergone phlebotomy (Fig. 1).
Staging of cancer
Patients who were diagnosed with a gastrointestinal
malignancy were staged according to the ‘tumor, node, metastasis’
(TNM) classification of malignant tumors from the International
Union Against Cancer, seventh edition, which is based on three
factors: primary tumor size, regional lymph node infiltration, and
distant metastasis (15). The
definition of curative treatment was curative surgery of stage
I–III gastric or colorectal cancer (16,17).
Ethics of the study
Approval for the study was obtained from the
hospital ethics committee of Asahi General Hospital. Information
regarding the study was provided to patients through the hospital
website, including the option to opt out. The study was
retrospective, so consent was not obtained prior to the study;
however, all data was anonymized.
Results
Causes of IDA
Of the 472 patients (239 men and 233 women) who were
diagnosed with IDA, 125 were omitted according to the exclusion
criteria (Fig. 1). In total, 347
patients at Asahi General Hospital were enrolled in the study
(Table I), of which 152 patients
(44%) were diagnosed by chance at the daily outpatient clinic
during treatment for other conditions, and 195 (56%) had visited
the hospital for specific symptoms or a check-up. The specific
symptoms included edema, shortness of breath, palpitation,
dizziness, loss of appetite, loss of consciousness and fever. In
total, 120 patients (25.4%) underwent both gastroscopy and
colonoscopy, 197 patients (41.7%) only underwent gastroscopy and 30
patients (6.4%) only underwent colonoscopy as part of their IDA
examination. Causes of IDA in this cohort are shown in Table II.
 | Table I.Characteristics of patients. |
Table I.
Characteristics of patients.
| Characteristics | All patients | All cancer types | Gastric cancer | Colorectal
cancer | Other cancer |
|---|
| Total, n | 347 | 50 | 24 | 23 | 3 |
| Sex, n (%) |
|
|
|
|
|
| Male | 193 (55.6) | 29 (58) | 18 (75) | 8 (35) | 3 (100) |
|
Female | 154 (44.4) | 21 (42) | 6 (25) | 15 (65) | 0 (0) |
| Age, mean years ±
standard deviation | 68.5±12.5 | 74.3±9.03 | 73.5±6.62 | 76.7±9.07 | 62.7±13.9 |
|
Males | 65.9±13.3 | 72.9±8.30 | 74.1±6.40 | 74.1±6.39 | 62.7±13.9 |
|
Females | 71.7±10.7 | 76.2±9.64 | 71.5±6.87 | 78.1±9.95 | – |
| Reason for visit, n
(%) |
|
|
|
|
|
|
Outpatient clinic | 152 (43.8) | 8 (16.0) | 4 (16.7) | 4 (17.4) | 0 |
|
Examination for anemia | 81 (23.3) | 9 (18.0) | 2 (8.33) | 7 (30.4) | 0 |
| Abdominal
symptoms | 30 (8.65) | 21 (42.0) | 12 (50.0) | 9 (39.1) | 0 |
| Fecal
occult blood | 2 (0.576) | 1 (2.00) | 0 | 1 (4.35) | 0 |
|
Others | 82 (23.6) | 11 (22.0) | 6 (25.0) | 2 (8.70) | 3 (100) |
| Table II.Causes of IDA. |
Table II.
Causes of IDA.
| Causes of IDA | Patients, n (%) |
|---|
| All | 347 (100) |
| Unknown | 148 (42.3) |
| Malignancy | 50 (14.3) |
| Gastrointestinal
bleeding | 50 (14.3) |
|
Post-gasterectomy | 41 (11.7) |
| Hemorrhoid | 17 (4.86) |
| Esophageal
varices | 12 (3.43) |
| Inflammatory bowel
disease | 5 (1.43) |
| Others | 24 (6.86) |
Characteristics of cancer
patients
A total of 50 (14.4%) cases of IDA in patients were
caused by malignancy; other causes included polyps, papilla tumor
and ischemic colitis. The characteristics of patients for whom
cancer was the cause of IDA are shown in Table I; 24 patients had gastric cancer and
23 patients had colorectal cancer. Other cancer types included 1
case of esophageal cancer and 2 of lymphoma. In total, 30% of the
patients diagnosed with cancer were asymptomatic, while others
experienced symptoms including shortness of breath, dizziness and
loss of appetite.
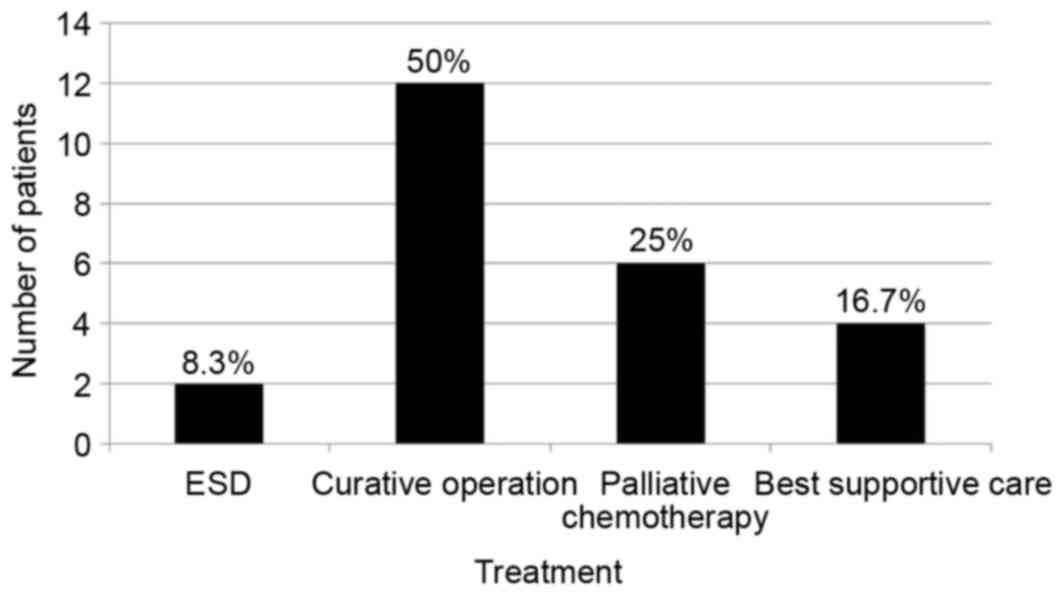
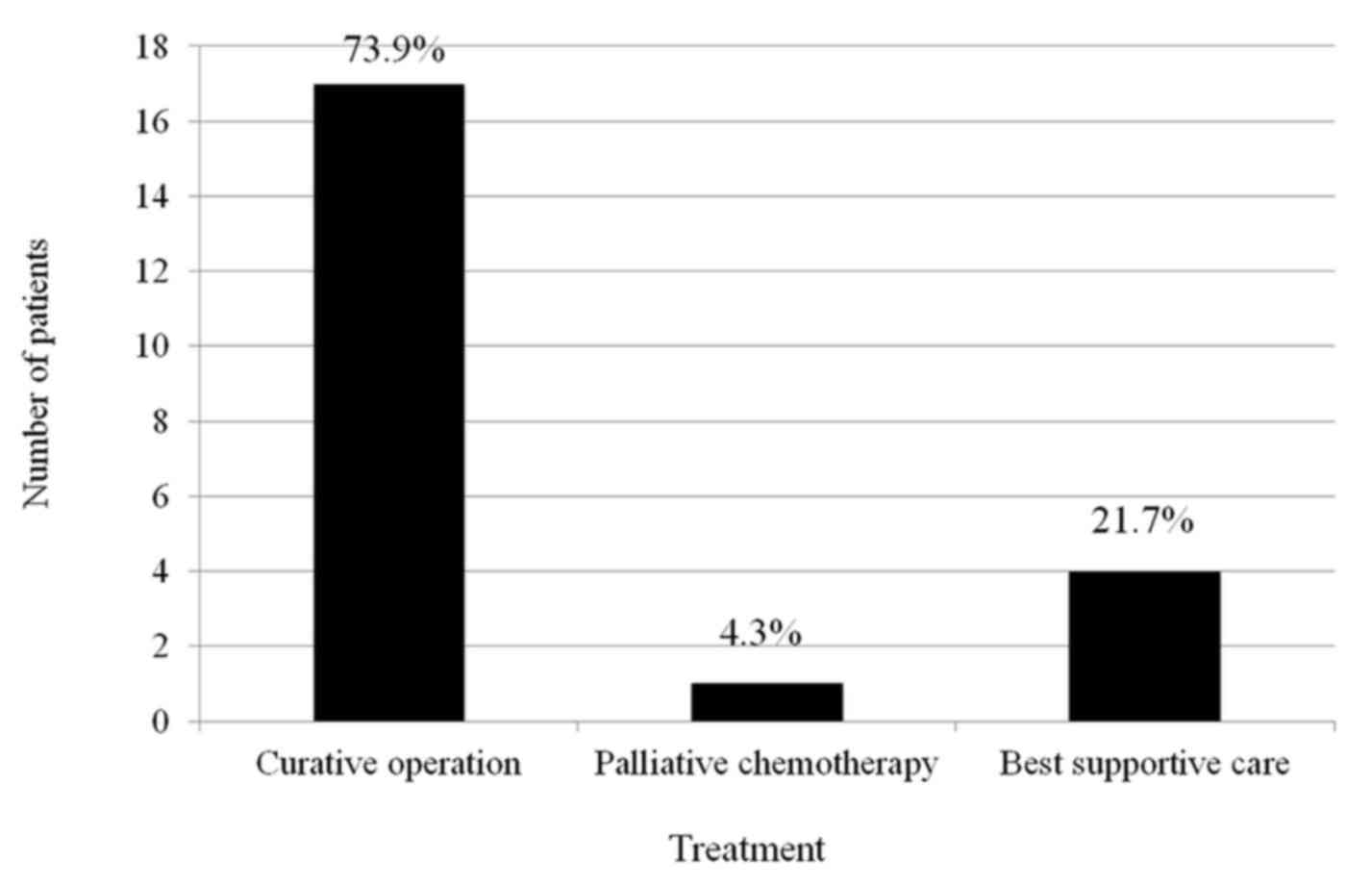
Staging and curative
resectability
The number of patients for each stage is shown in
Table III. Curative surgery,
including endoscopic treatment, was performed on 14 gastric cancer
patients (58.3%) and 17 colorectal cancer patients (74.0%).
Subsequently, 1 gastric cancer patient and 2 colorectal cancer
patients refused further examination for staging. The treatment
results of cancer patients are shown in Figs. 2 and 3.
| Table III.Staging of cancer patients. |
Table III.
Staging of cancer patients.
| Staging | Gastric cancer, n
(%) | Colorectal cancer, n
(%) |
|---|
| All | 23 | 21 |
| I | 6 (26.1) | 0 (0) |
| II | 3 (13.0) | 9 (42.9) |
| III | 5 (21.7) | 8 (38.1) |
| IV | 9 (39.1) | 4 (19.0) |
Discussion
The present study is the first report on the staging
and resectability of gastrointestinal cancer cases identified
following the examination of patients with IDA in Japan. The
present study revealed that a full investigation for the cause of
IDA occurs in <30% of cases in the practice. Despite the low
frequency of investigation, investigations that were performed
demonstrated that malignancy was the cause of IDA in 50 patients
(14.4%), which is in accordance with data in previous studies
(2,5,18).
Given that colorectal cancer is observed at a much
higher rate compared with gastric cancer in Western countries,
recommendations often suggest a colonoscopy should be performed at
first for IDA patients who are >50 years of age, followed by a
gastroscopy if no cause is revealed (19,20). For
example, Wilcox et al (18)
designed a prospective clinical study for IDA in which colonoscopy
is followed by gastroscopy. In contrast, a study in Taiwan reported
an equal number of gastric and colorectal cancer diagnoses
(5), while a study in Korea
identified that gastric cancer cases were much more frequent than
colorectal cancer cases (21). This
discrepancy may have resulted from geographical differences, as
colorectal cancer is observed at a much higher rate than gastric
cancer in western countries. This may suggest a need for the
consideration of geographical and ethnic differences in an approach
to IDA (21). The present study,
based on data from Japan, demonstrated approximately equal numbers
of gastric and colorectal cancer patients. Taken together, this
evidence suggests that in Asian countries, gastric cancer is more
likely to be a cause of IDA compared with Western countries.
From the prospect of staging and resectability, 60%
of patients who had their cancer detected through IDA examination
presented with cancer that was at stage III or less, based on the
TNM classification system, and therefore exhibited curative
resectability. Gastrointestinal cancer may lead to IDA by causing
chronic inflammation and active chronic bleeding, associated with
ulcer formation (22). Based on this
concept, cancer may be found prior to metastasis at a resectable
stage when endoscopy is performed on IDA patients. This is
supported by the present study; numerous patients presented with
gastrointestinal cancer suitable for curative surgery despite the
malignancy being identified in examinations for IDA. Thus, even
when patients cannot receive a full check-up for further
investigation of IDA, examination for the detection of cancer is
highly recommended based on the present study. As modern capsule
endoscopy and CT colonography techniques also contribute to the
detection of cancer (23,24), a combination of these different
modalities is recommended to allow an increased rate of
gastrointestinal malignancies to be detected in patients with
IDA.
The limitation of the present study is its
retrospective nature; not all the patients who visited the hospital
during the period were examined for IDA, which would be the ideal
procedure for a study on IDA-associated malignancy.
In conclusion, in the present study, malignancies
were found in 50 patients with IDA (14.4%). 24 of these patients
exhibited gastric cancer while 23 exhibited colorectal cancer. The
majority of the cancers were resectable, and curative surgery,
including endoscopic treatment, was performed. The preparation of a
practical IDA investigation program consisting of several
modalities is required.
References
|
1
|
McLean E, Cogswell M, Egli I, Wojdyla D
and de Benoist B: Worldwide prevalence of anaemia, WHO vitamin and
mineral nutrition information system, 1993–2005. Public Health
Nutr. 12:444–454. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Rockey DC and Cello JP: Evaluation of the
gastrointestinal tract in patients with iron-deficiency anemia. N
Engl J Med. 329:1691–1695. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Goddard AF, McIntyre AS and Scott BB:
Guidelines for the management of iron deficiency anaemia. British
Society of Gastroenterology. Gut. 46:(Suppl 3–4). IV1–IV5. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Lindsay JO, Robinson SD, Jackson JE and
Walters JR: The investigation of iron deficiency anemia-a hospital
based audit. Hepatogastroenterology. 46:2887–2890. 1999.PubMed/NCBI
|
|
5
|
Ho CH, Chau WK, Hsu HC, Gau JP, You JY and
Chen CC: Predictive risk factors and prevalence of malignancy in
patients with iron deficiency anemia in Taiwan. Am J Hematol.
78:108–112. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
James MW, Chen CM, Goddard WP, Scott BB
and Goddard AF: Risk factors for gastrointestinal malignancy in
patients with iron-deficiency anaemia. Eur J Gastroenterol Hepatol.
17:1197–1203. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Napal JJ, Hernández JL, Alonso J and
Casuso E: Differential factors of tumor etiology for iron
deficiency anemia of probable gastrointestinal origin. Rev Clin
Esp. 209:265–269. 2009.(In Spanish). View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Droogendijk J, Beukers R, Berendes PB, Tax
MG, Sonnenveld P and Levin MD: Screening for gastrointestinal
malignancy in patients with iron deficiency anemia by general
practitioners: An observational study. Scand J Gastroenterol.
46:1105–1110. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Khadem G, Scott IA and Klein K: Evaluation
of iron deficiency anaemia in tertiary hospital settings: Room for
improvement? Intern Med J. 42:658–664. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Gomollon F and Gisbert JP: Anemia and
digestive diseases: An update for the clinician. World J
Gastroenterol. 15:4615–4626. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Domínguez-Ayala M, Díez-Vallejo J and
Comas-Fuentes A: Missed opportunities in early diagnosis of
symptomatic colorectal cancer. Rev Esp Enferm Dig. 104:343–349.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Stagnitti A, Barchetti F, Barchetti G,
Pasqualitto E, Sartori A, Glorioso M, Gigli S, Buonocore V, Monti
ML, Marini A, et al: Preoperative staging of colorectal cancer
using virtual colonoscopy: Correlation with surgical results. Eur
Rev Med Pharmacol Sci. 19:1645–1651. 2015.PubMed/NCBI
|
|
13
|
Guyatt GH, Oxman AD, Ali M, Willian A,
Mcllroy W and Patterson C: Laboratory diagnosis of iron-deficiency
anemia: An overview. J Gen Intern Med. 7:145–153. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Mankodi S, Hayee BH, O'Donohue J and
Reffitt D: Anaemia investigation in practice: Inappropriate, cost
inefficient with a risk of missing gastrointestinal cancer. Can we
improve? Clin Med (Lond). 10:115–118. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Sobin LH, Gospodarowicz MK and Wittekind
C: TNM Classification of Malignant Tumours7. John Wiley & Sons.
Incorporated; pp. 74–77. 102–105. 2011
|
|
16
|
Benson AB 3rd, Venook AP, Cederquist L,
Chan E, Chen YJ, Cooper HS, Deming D, Engstrom PF, Enzinger PC,
Fichera A, et al: Colon Cancer, Version 1, 2017, NCCN Clinical
Practice Guidelines in Oncology. J Natl Compr Canc Netw. 3:370–398.
2017. View Article : Google Scholar
|
|
17
|
Ajani JA, D'Amico TA, Almhanna K, Bentrem
DJ, Chao J, Das P, Denlinger CS, Fanta P, Farjah F, Fuchs CS, et
al: Gastric Cancer, Version 3.2016, NCCN Clinical Practice
Guidelines in Oncology. J Natl Compr Canc Netw. 10:1286–1312. 2016.
View Article : Google Scholar
|
|
18
|
Wilcox CM, Alexander LN, Straub RF and
Clark WS: A prospective endoscopic evaluation of the causes of
upper GI hemorrhage in alcoholics: A focus on alcoholic
gastropathy. Am J Gastroenterol. 91:1343–1347. 1996.PubMed/NCBI
|
|
19
|
Sayer JM and Long RG: A perspective on
iron deficiency anemia. Gut. 34:1297–1299. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Killip S, Bennett JM and Chambers MD: Iron
deficiency anemia. Am Fam Physician. 75:671–678. 2007.PubMed/NCBI
|
|
21
|
Yun GW, Yang YJ, Song IC, Park KU, Baek
SW, Yun HJ, Kim S, Jo DY and Lee HJ: A prospective evaluation of
adult men with iron-deficiency anemia in Korea. Intern Med.
50:1371–1375. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Logan EC, Yates JM, Stewart RM, Fielding K
and Kendrick D: Investigation and management of iron deficiency
anaemia in general practice: A cluster randomised controlled trial
of a simple management prompt. Postgrad Med J. 78:533–537. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Johnson CD, Chen MH, Toledano AY, Heiken
JP, Dachman A, Kuo MD, Menias CO, Siewert B, Cheema JI, Obregon RG,
et al: Accuracy of CT colonography for detection of large adenomas
and cancers. N Engl J Med. 359:1207–1217. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Van Gossum A, Munoz-Navas M,
Fernandez-Urien I, Carretero C, Gay G, Delvaux M, Lapalus MG,
Ponchon T, Neuhaus H, Philipper M, et al: Capsule endoscopy versus
colonoscopy for the detection of polyps and cancer. N Engl J Med.
361:264–270. 2009. View Article : Google Scholar : PubMed/NCBI
|