Introduction
In the last century, primary tumors of the patella
are uncommon and account for <0.12% of bone tumors in the United
States (1). The incidence of
metastatic lesions to the patella is even lower (2). A Medline search from of studies
published between 1960 and 2016 yielded 44 reported cases of
patellar metastases. Primary tumors that have been reported to
metastasize to the patella include carcinomas of the lung, kidney,
breast, esophagus, uterine cervix, skin (malignant melanoma),
bowel, larynx, head and neck. The reported cases of patellar
metastases are presented in Table I.
Of these 44 cases, >10 presented with anterior knee pain as the
first manifestation (3–11). The mean age of the patients at
presentation was 57 years (range, 37–86 years). The present study
analyzed these cases of primary sites of patellar metastasis. In
the present study, the metastatic patellar tumors were classified
according to the primary site and type. A detailed summary and
description is presented.
 | Table I.Summary of the reported cases of
patellar metastasis. |
Table I.
Summary of the reported cases of
patellar metastasis.
| Site of primary
tumor | Case | Mean average age,
years | Sex | Clinical
presentation | Radiological
appearance | Treatment | (Refs.) |
|---|
| Lung | 17 | 64.8 | M12, W2, N3 | Knee pain and
swelling | Osteolytic lesion
of patella; increased uptake of radioisotope; a mass in the
lobe | Patellectomy and
reconstruction of the extensor mechanism; wide excision | (3–6,9,10,12–14,16–23) |
| Kidney | 5 | 59.4 | M4, W1 | Knee pain and
swelling; hematuria, loin pain and loin mass (10%) | Osteolytic lesion,
lucent area and cortical disruption of patella; increased uptake of
radioisotope; a mass arising from the superior pole of the
kidney | Radical nephrectomy
and patellectomy; radiotherapy and chemical adjuvant (zolendronic
acid) treatment | (7,8,11,25,27) |
| Breast | 3 | 48 | W1, N2 | Knee pain and
swelling; a lump in the breast | Osteolytic lesion
of patella; trabecular destruction and transverse crack | Patellectomy;
radiotherapy | (29–31) |
| Esophagus | 2 | 53.5 | M2 | Progressive
dysphagia and weight loss; knee pain and swelling | Esophageal mass; a
lytic destruction of patella and a mass in the suprapatellar
bursa | Esophagectomy or
esophagogastrostomy; patellectomy; radiotherapy | (32,33) |
| Skin
(melanoma) | 3 | 55 | M1, W2 | Knee pain and
swelling | Mixed lytic and
blastic lesions of the patella; increased [18F]
fluorodeoxyglucose accumulation in the posterior of patella | Patellectomy;
radiotherapy; chemotherapy (temozolomide) | (32,39,40) |
| Colon | 4 | 54.3 | M2, W1, N1 | Knee pain and
swelling | Osteolytic lesion
of patella; increased uptake of radioisotope; the niche showed by
barium enema examination | Synovial resection
and a patellectomy; radiotherapy | (32,35–37) |
| Uterine cervix | 2 | 51.5 | W2 | Post-coital
bleeding; knee pain and swelling | Joint effusion;
demineralization of the bones of the knee | Radiotherapy | (32,34) |
Carcinoma of the lung
The review of the literature revealed that
metastasis from lung carcinoma is most common, with 40% of all
patellar metastases originating from a primary tumor located in the
lung. In total, 7 cases were associated with squamous cell
carcinoma (4,5,9,10,12–15) and 7
cases with adenocarcinoma (3,16–21). Only
1 case was adenosquamous (6), whereas
for 2 cases, the histological type of lung cancer was not stated
(22,23). It is common for adenocarcinoma of the
lung to give rise to remote metastasis prior to the onset of
pulmonary symptoms, which may be attributed to the peripheral
pulmonary growth of the tumor. By contrast, metastasis from lung
squamous or epidermoid carcinoma is not common since these tumors
are usually centrally located and therefore present with pulmonary
symptoms (6).
Clinically, metastasis of the patella accompanied by
knee pain was the presenting symptom of lung cancer in the
patients. The common early manifestation of lung cancer is a cough
and sputum production (~75% patients), whereas bone pain as an
initial symptom occurred in 22% of the patients (24). Patients who had patellar metastasis of
the lung presented with progressive knee pain and limited mobility
that was relieved by analgesic drugs (10). The patients frequently had a history
of smoking along with a persistent cough and weight loss (3,5,12,14,17,22).
Additionally, 2 patients had recent trauma history (3,9).
On physical examination, the diseased knee was
euthermic, swollen, and tested positive in patellar shock and
grinding tests (6,10). A single patient exhibited inflammatory
signs in the diseased knee (3). Upon
palpation, the patellofemoral joint was moderately painful compared
with the healthy side. Patients usually exhibited limited
flexibility of the affected knee, with atrophy of the quadriceps
(5). Additionally, the sounds of
breathing were diminished over the pulmonary lesion when observed
using auscultation (10,12). Certain patients did not exhibit any
symptoms of respiratory distress.
In the majority of the patients, all routine blood
tests including erythrocyte sedimentation rate (ESR), C-reactive
protein (CRP), acid phosphatase (ACP) and alkaline phosphatase
(ALP) were within normal range (6).
In a single case, the level of ESR was increased and a normochromic
anemia was observed (5). Another case
had an increased level of ACP (10).
Serum ALP level was increased in a patient with monoarticular
arthritis secondary to metastatic patellar spread of bronchogenic
carcinoma (15). A Mantoux test may
exclude the possibility of tuberculosis in the knee (12).
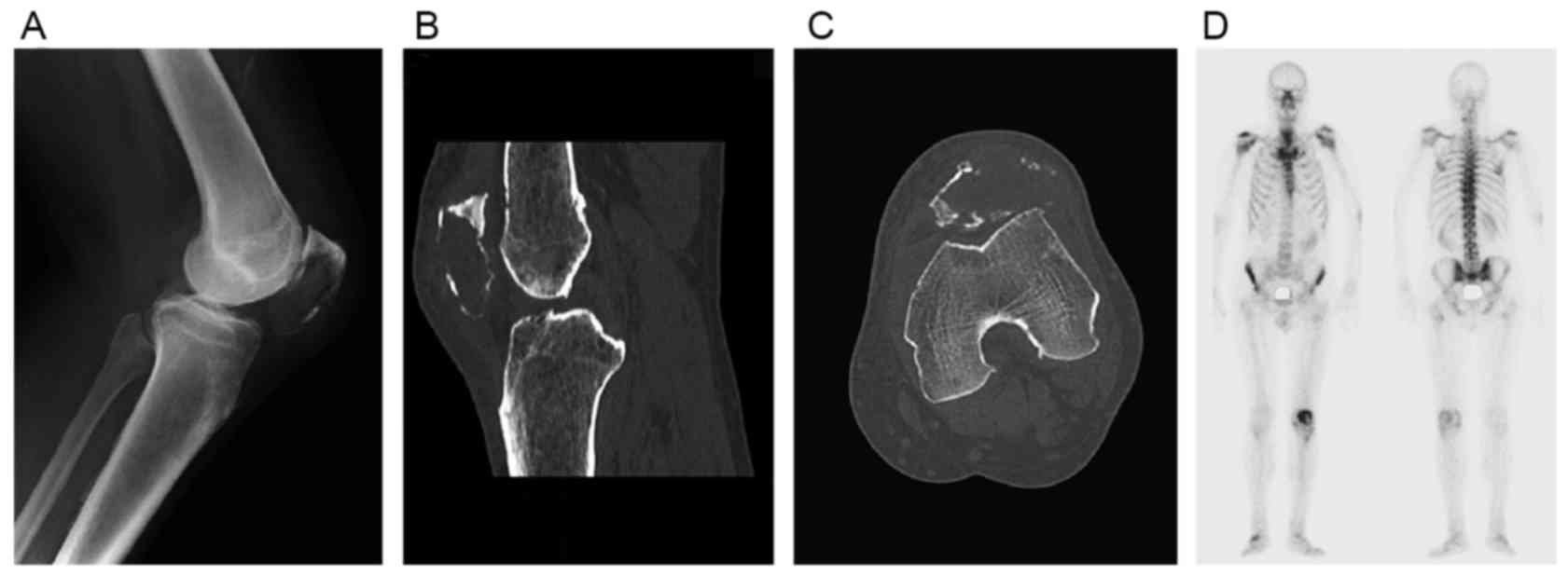
Radiographic examination of the knee commonly
revealed mild osteoarthritis with a cystic lesion in the patella
(Fig. 1A). The result of computed
tomography (CT) imaging (Fig. 1B and
C) may also indicate an extended osteolytic lesion (6). Bone scintigraphy (Fig. 1D) may reveal an increased uptake of
radioisotope in the affected patella. The use of
[18F]fluorodeoxyglucose positron emission
tomography/computed tomography (PET-CT) and single photon emission
tomography/computed tomography were not considered to be valuable
tools for the evaluation of the malignant tumors (13,16).
However, the PET-CT showed a hypercaptation of the pulmonary
lesions, of a conglomerate lymph node mass in the hilum and of the
patellar lesion, suggestive of active metastatic disease.
Arthroscopy was helpful to provide insight into the intra-articular
situation including synovial effusion and general degenerative
changes. On occasion, soft blue cartilage was indicative of the
pathological change. The radiographs of the chest, bronchoscope and
thoracic multi-slice computed tomography were necessary for
diagnosis of the primary lesion, since it was possible to easily
identify a mass in the lobe (6,13,22,25).
Excision biopsy was performed and the diagnosis was confirmed using
pathological testing. Immunohistochemically, the ceroplastic cells
co-expressed keratin and vimentin. Carcinoembryonic antigen (CEA)
and epithelial membrane antigen (EMA) were also present in certain
cases. Thyroid transcription factor-1 (TTF-1) confirmed the nuclear
positivity in the majority of adenocarcinoma cells, which was
suggestive of the primary lung process. However, the squamous cells
were TTF-1-negative and cytokeratin 5/6-positive which confirmed
the adenosquamous nature of the lung carcinoma (6).
For patellar malignant tumors, surgery was the
optimal therapeutic option. The treatment of patellar metastasis is
dependent on the size of the lesion. Early deposits without
soft-tissue extension may be treated by patellectomy and
reconstruction of the extensor mechanism (6,13,16). Postoperatively, the patients wore a
knee immobilizer (9). Nevertheless,
larger lesions with soft-tissue extension required a wide excision,
followed by systemic chemotherapy and local radiation therapy
(16). In one case, the size of the
lesion was >50% of the patella and the anterior cortex was not
intact. Aktas et al (10)
adopted total patellectomy and total synovial resection for
diagnostic and therapeutic purposes. This may help patients to
improve their quality of life by eliminating severe pain and
disability (10). The majority of the
patients succumbed to progressive lung disease within a short
postoperative period (3,9,10,14,15,17).
However, 2 patients presented asymptomatically and were capable of
full functioning of the knee with no recurrence (6,13).
Carcinoma of the kidney
The cases of metastatic tumor from renal cell
carcinoma (RCC) account for 14% of all patellar metastases. Howlett
and Caranasos (25) described a
patient with an arteriovenous shunt secondary to metastatic
patellar spread of renal carcinoma.
Clinically, ~30% of patients with RCC present with
symptoms. It is associated with metastatic disease. The classic
symptomatic triad of hematuria, loin pain and loin mass is uncommon
(10%) and only observed in advanced cases (26). Long-term knee pain was the main
complaint of the patients, who were often no longer able to walk or
move. There was only one case with associated trauma (8).
Additionally, 1 patient presented with knee pain due
to a pathological fracture (27). A
physical examination of the affected knee revealed swelling,
tenderness, mild erythema and painful flexion-extension motion
(7,8,27). No
other notable physical results were observed.
Laboratory investigations including a full blood
count, routine biochemistry, ESR, CRP and prostate-specific antigen
(PSA) levels did not reveal any notable abnormalities (8).
X-ray (Fig. 2A)
revealed a lucency within the patella and a discontinuity in the
cortex of the patella with an osteolytic lesion (7,8,11,27). CT
imaging (Fig. 2B and C) identified a
large lucent area occupying the majority of the patella with
multiple areas of cortical disruption along its border (7,8). A
radioisotope bone scan (Fig. 2D)
revealed isolated abnormal tracer activity local to the patella
(7). A renal ultrasound revealed a
large mass arising from the superior pole of the kidney (7). Subsequent CT scanning of the chest,
abdomen and pelvis contributed to the diagnosis of the primary
lesion and identified the stage of disease; a mass was easily
located in the pole of the kidney. The appearance of the mass was
consistent with a primary RCC. Histological examination of the
resected patella indicated metastatic renal adenocarcinoma.
Surgery remains the main method of treatment. A
radical nephrectomy and patellectomy were performed, which may be
crucial as there was no evidence of other metastases, although the
presentation as a pathological fracture may make dissemination
easier (7,8,27). Lim
et al (8) adopted cryotherapy
to realize a unique anatomical preservation on the basis of two
principles. First, the treatment is suitable for the patient with a
short life expectancy on the basis of the American Joint Committee
on Cancer (AJCC) Staging for stage 4 RCC. Secondly, RCC metastasis
presents a unique histological type of bony metastasis in which
disease control concepts appear to be similar to primary bone
disease, with no survival rate advantage achieved by performing a
wide resection as opposed to intralesional curettage and local
stabilization (8,28). In addition, radiotherapy and chemical
adjuvant (zolendronic acid) treatment for the patellar metastasis
were reported in several cases (7).
Postoperatively, the patients exhibited no evidence of progressive
disease and were capable of full motion of the affected knee
(8,11). Additionally, 2 patients accepted a
conservative treatment that was not well-described in the report.
There was no further information regarding follow-up (7,25).
Carcinoma of the breast
Patellar metastases originating from breast tumors
are uncommon with an incidence of ~2% among all patellar
metastases.
Clinically, a lump or a change in the shape of the
breast may be the first observable manifestation in the patients
(29,30). Specific cases may exhibit progressive
knee pain, swelling and erythema (31). However, none of the patients had a
history of knee trauma or signs of inflammation.
Upon physical examination, a change in the size or
shape of the breast may be observed and a lump in the breast felt
(29). The patient may exhibit
swelling, tenderness, moderate effusion and decreased range of
motion in the affected knee (31).
The majority of routine laboratory findings were within normal
ranges.
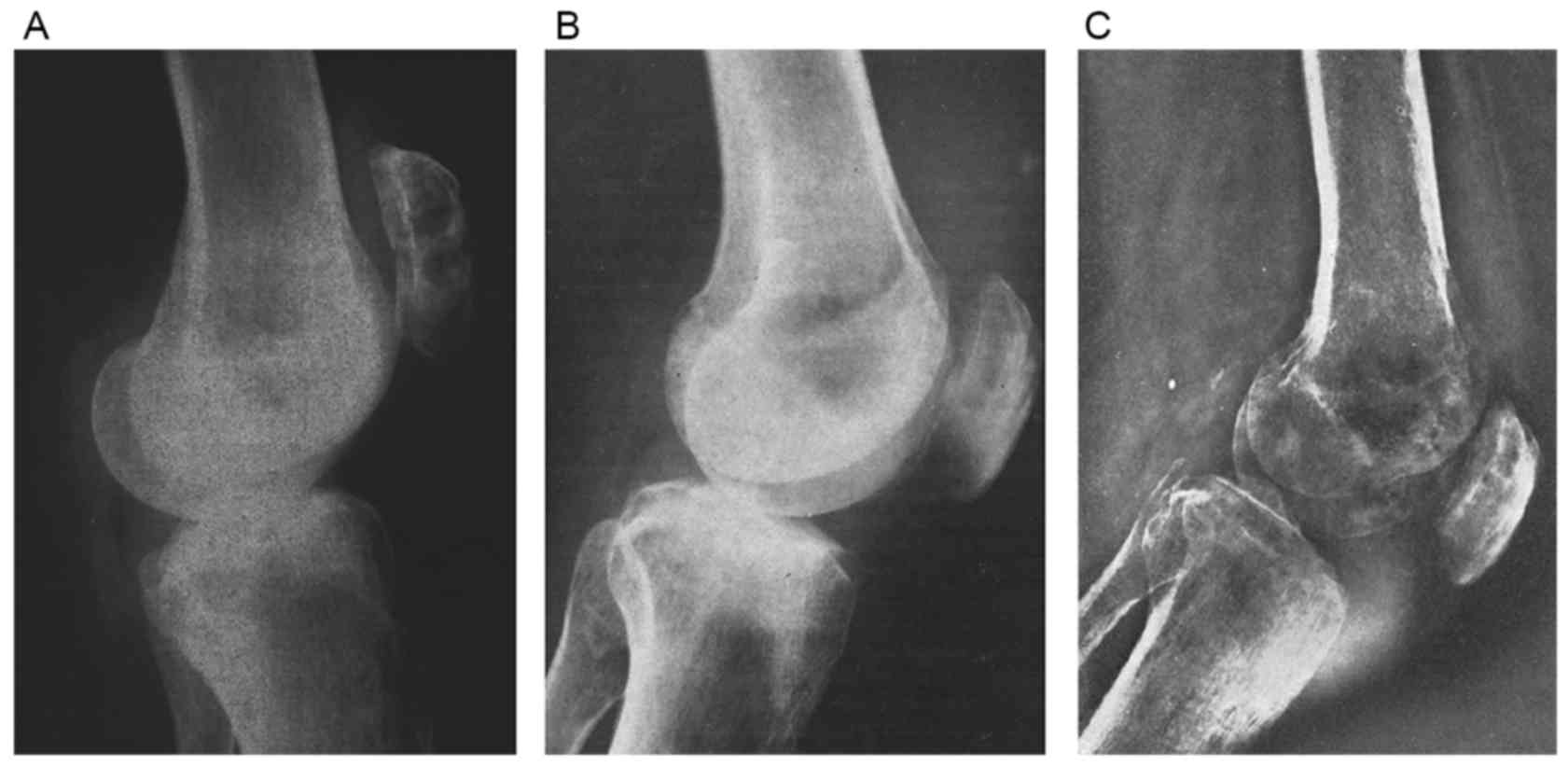
Radiographs (Fig. 3A)
demonstrated osteolytic deposits and an area of trabecular
destruction of the patella (31).
Mammogram, ultrasound and bone scintigraphy were meaningful to the
determination of the patellar metastasis.
Histological examination revealed that the
spheroidal cells replacing the trabecular bone of the patella and
filling the center of the field with normal bone on either side
were similar to those in the primary breast carcinoma.
A patellectomy was performed followed by routine
physiotherapy. Radiotherapy was used to target the internal mammary
and mediastinum, with Prednisone supplemented. The knee pain was
relieved and effusion was gradually aspirated. The general
condition of 1 case deteriorated rapidly and the patient succumbed
following a short period of time (31).
Carcinoma of the esophagus
Metastasizing from the esophagus is rare, with an
incidence of 5% of all patellar metastases.
Normally, the patients initially had a history of
progressive dysphagia and weight loss. Immobilizing pain, swelling
and effusion in the affected knee developed gradually (32,33).
Physical examination revealed considerable swelling,
warmth and knee pain (32,33). Patients typically had a limited range
motion of the affected knee. Certain patients did not seek medical
attention until pain and disability became deteriorative (33). Results of routine laboratory studies,
including blood cell count, ESR, blood calcium and ALP, were
demonstrated to be normal (32).
Radiographs (Fig. 3B)
of the knee presented a lytic lesion, demineralization of the
patella and a mass in the suprapatellar bursa. An arthrogram and
arteriography demonstrates the marked vascularity in the areas of
irregular synovium which contained the metastatic nodules (32,33). An
arthrocentesis collected synovial fluid contaminated with blood,
which yielded Staphylococcus aureus in culture. A
barium-swallow examination and esophagoscopy revealed an esophageal
mass. Following the examination of a tissue biopsy, the mass was
revealed to be an epidermoid carcinoma (33). Stoler and Staple (32) reported that a closed patellar biopsy,
two Cope needle biopsies of the synovium and cytology of the joint
fluid may be used for the diagnosis. However, an open patellar
biopsy or arthrotomy may be recommended when the results were
negative (32,33).
Metastatic epidermoid carcinoma consistent with an
esophageal origin was confirmed in permanent pathological
sections.
The optimal treatment approach remains unknown.
Ashby and Dapper (33) promoted a
surgical approach. In 1 case, an esophagectomy and
esophagogastrostomy were performed following a total patellectomy.
In the postoperative period, radiation therapy was valuable in the
relief of pain. However, Stoler and Staple (32) indicated a conservative treatment that
was not well-described in the report. The 2 cases had no
follow-up.
Carcinoma of the uterine cervix
Metastasizing from uterine cervix is rare (~2% of
all patellar metastases), and only a small number of cases of this
type was reported.
Generally, the patients presented with post-coital
bleeding (32). The pain, swelling
and progressive disability of the affected knee may often disturb
the patients (32,34).
Upon physical examination, symptoms including
warmth, swelling and tenderness of the patella were observed. There
was redness and a localized increase in temperature. The range of
motion was limited. Occasionally, clinical examination could not be
entirely completed due to severe pain (34). No other joints were affected.
Routine laboratory studies and ESR of reported cases
were normal (32). Radiographs of the
diseased knee (Fig. 3C) revealed
minimal joint effusion, lytic destruction and demineralization of
the bones of the knee (32). An open
biopsy of the synovium and patella determined metastatic epidermoid
carcinoma. Stoler et al (32)
reported that radiation therapy is the treatment of choice and it
provides significant symptomatic relief.
Carcinoma of the colon
Metastasizing from colon is rare, with an incidence
of ~9% of all patellar metastases.
Clinically, the patients always presented with
increasing knee pain accompanied by swelling (32,35–37), which
persistently affected mobility. Furthermore, 1 case was associated
with traumatic history and aggravated by motion (36).
Upon physical examination, warmth, tenderness,
swelling and limited extension of the diseased knee were observed
(32,36,37). No
other joints were involved and examination of the other knee was
not remarkable. Routine laboratory studies revealed that ESR and
CEA levels were within normal ranges (35,36).
Radiographs revealed osteolytic lesions and
destruction of the subchondral bone of the patella. Further
radiography studies may demonstrate a lytic lesion in the skull or
a mass in the lung. Bone scintigraphy revealed dense hyperfixation
of the affected patella (36). Barium
enema examination revealed a lesion in the midsigmoid colon
suggesting the presence of a tumor (32). Arthrotomy was performed and revealed
that the patella was markedly friable, although the synovium was
normal. Pathological examination of the biopsy, stained with
hematoxylin-eosin-safran, revealed the diagnosis of patellar
metastasis from a well-differentiated large bowel adenocarcinoma
(36).
Urvoy et al (36) were in favor of surgical treatment. A
partial colectomy was performed followed by a total patellectomy
and extensive synovial resection according to the technique of Boyd
and Hawkin (38). Following surgery,
the patient was asymptomatic and capable of full functioning of the
affected knee. Postoperative radiotherapy was administered to
complement the surgical treatment (36). However, Stoler and Staple (32) reported that the patient was treated
only with radiotherapy and discharged. The treatment of the other
cases was not well-described in the report.
Malignant melanoma
The tumors originating from malignant melanoma
account for ~7% of all patellar metastases. Melanoma is well-known
for its capacity to metastasize to numerous sites, including
certain places rarely observed with other solid tumors.
Clinically, the patients presented with increasing
anterior knee pain and swelling in the affected knee (32,39,40).
Patients were not able to bear weight on the affected leg for more
than a short period of time. Only 1 case had a relevant medical
history of a melanoma on the back and underwent wide excision of
lesion followed by lymphadenectomy (40).
Upon physical examination, symptoms including mild
pain, mass, swelling, tenderness, heat and limited motion of the
patellar were observed (32,39,40).
Furthermore, the quadriceps muscle was atrophied (39). In 2 cases, multiple metastases were
established in lymph nodes of different regions (32).
Routine laboratory studies revealed that ESR and
other blood tests were within normal ranges. However, 1 case
revealed an increase in the white blood cell count and plasma
(39).
A radiograph of the affected knee demonstrated mixed
lytic and blastic lesions of the patella. The cortex was intact
without periosteal reaction (39). A
chest X-ray revealed large basal opacities suggestive of multiple
metastases (39). PET-CT was
performed to investigate metastatic areas. Increased [18
F]fluorodeoxyglucose accumulation in the patella was observed with
an abnormal standardized uptake rate (40).
Histopathological examination of the skin biopsy
revealed a superficial spreading type of malignant melanoma with an
invasion; the changes in the patella confirmed metastatic malignant
melanoma (39).
Treatment options for the tumor originating from
malignant melanoma remain in dispute. Jaeger et al (39) were in favor of a surgical approach. A
patellectomy was performed on a patient and the pain in the
affected knee was relieved. In the postoperative period, the
condition of the patient deteriorated with weight loss, diarrhea
and generalized abdominal tenderness. The patient succumbed
following a short period of time. Tas and Keskin (40) reported that the patient was treated
with single-agent temozolomide chemotherapy. In another case, the
patient was treated conservatively and discharged (32). The 2 cases had no follow-up.
Other primary tumors
Other primary tumors metastasizing to the patella
were also reported, including carcinoma of prostate (41), malignant lymphoma (42,43),
laryngeal squamous cell carcinoma (44), floor of the mouth (45), salivary gland and extramammary Paget's
disease with invasive carcinoma (46).
Discussion
Metastasis of any type to the patella is rare in
comparison with primary tumors of the patella. Case reports and the
associated review articles of the primary patellar tumors may be
easily searched (47). Nevertheless,
only a small number of reports related to patellar metastasis has
been published in the scientific literature.
The patella stems from a cartilaginous precursor in
the third month of gestation and ossifies at ~3 years of age. Its
ossification is similar to that of an epiphysis or apophysis of a
long bone. This makes the patella a possible site of bony lesions
(2). The patella is a sesamoid bone
with a relatively poor vascular supply, consisting of a number of
nutrient branches from the collateral vessels of the knee. Thus,
patellar circulation may not be sufficient for tumor cells to occur
and metastasize (48). Furthermore,
the small size of the patella and its dense cancellous structure
make the bone an unlikely site for a metastatic deposit. Sosnoski
et al (49) revealed that
trauma may be a factor in determining the establishment of a
circulating tumor embolus. Although the theory illustrating
patellar metastases has reached an agreement in the majority of the
literature, there remains another hypothesis. Lim et al
(8) reported that the tumor emboli
did not exhibit preferential metastasis to highly vascularized
bones including the lumbar spine. This raises the consideration of
tissue tropism as another aspect influencing carcinogenesis
(50). A previous study revealed that
the probability of disease-free and overall survival rates in
colorectal cancer was dependent on lymph node metastasis and the
degree of tumor differentiation, but not on the presence of
circulating tumor cells (51). Tissue
tropism has previously become a focus as another important factor
in tumor metastases. Kang (52)
demonstrated the development of mutations allowing metastasis in a
targeted tissue-specific manner in one experiment. The author
insisted that it is possible that the patient may possess a
molecular make-up of the primary tumor enabling preferential
metastasis to the patella. Therefore, further molecular studies are
required in order to determine the tumor tropism of the primary
deposits.
In the review of the literature, there were ~20
patients with patellar metastasis (lung, kidney, breast, esophagus,
uterine cervix, colon and skin) in the left knee compared with 9
cases in the right side. For potential patients suffering from left
patellar tumors, more attention should be paid to the possible
diagnosis of patellar metastasis.
The most common symptom of patellar metastases is
anterior knee pain that usually lasts a marked period of time from
pain onset to determination via diagnosis. In certain cases, it is
the only sign of the patellar metastases. Certain patients complain
of immediate patellar pain following unimpressive injury that may
be the result of a pathological fracture. Swelling is the second
most common symptom and occurs in multiple cases of patellar
tumors. The impaired function of flexion and extension upon
physical examination is easier to determine. Affected by pain and
swelling, the range of motion of the diseased knee is decreased.
With the limitation of motion and limp, patients may experience
muscular atrophy of the quadriceps. Additionally, tumor mass is
another symptom which is often revealed through palpation during a
physical examination. It is not only primary malignancies but also
aggressive tumors of the patella which are able to raise local
redness, heat, effusion and other inflammatory responses.
Furthermore, it is hypothesized that there may be an association
between the lesion site and the tumor type. However, with
asymptomatic knee lesions, patients may present with the typical
symptoms of the primary tumor site, including cough and sputum of
lung tumors, progressive dysphagia and weight loss of esophageal
tumor and breast lump of the breast tumor. When signs of weight
loss, night sweats and other cachexia appear, the possibility of
other malignant tumors should be considered.
However, more evidence is required to distinguish
patellar metastases from primary tumors and other types of lesion.
In a clinical setting, a painful swollen knee is commonly
associated with septic arthritis, rheumatic arthritis and
degenerative osteoarthritis. Certain authors described knee
symptoms as marked. Although a tumor is not a frequently suspected
cause of anterior knee pain, the possibility of patella metastasis
should not be ignored in patients with malignancy. As the patellar
neoplasm is such a rare etiology as anterior knee pain, the
determination is often postponed.
In patients suffering anterior knee pain, a
radiograph is the most common method to identify patellar anomalies
and may contribute to the early diagnosis of a patellar tumor
(53). The traits of the X-ray
including bone destruction, extent, margins, cortex, sclerotic rim,
calcifications, ossification, periosteal reaction, pathological
fracture and surrounding involvement should be considered
carefully. Malignant tumors are frequently identified with
periosteal reaction, permeative destruction, total patellar
extension and ossifications or pathological fracture. Occasionally,
radiographic diagnosis is insufficient due to metastatic cancer,
Paget's disease, plasmacytoma, osteomyelitis, tuberculosis
hyperparathyroidism, gout and other lytic neoplastic lesions of the
patella. Compared with plain radiograph, bone scintigraphy is more
useful in the early diagnosis of bone metastasis. Primary patellar
tumors are often not studied through imaging results, which are
otherwise helpful to determine the stage of the lesion and the
appropriate surgical course. The combination of X-ray, CT, MRI and
PET-CT is particularly necessary for determination of diagnosis,
involvement of the surrounding tissue and precise tumor location.
Furthermore, a bone scan appears to lack the sensitivity required
to indicate patellar tumors. Only a small number of the cases were
identified with an increased focal activity on the lesion. In
addition, according to the primary symptoms, chest radiograph,
abdominal CT, renal ultrasound or barium enema examination is
recommended for all the patients with patellar tumors. This is
meaningful for determining diagnosis as well as guiding treatment
plan.
Owing to the rarity of reports and unusual changes,
the reported reviews of laboratory tests on the patellar tumors
remain limited. With the increase in relative cases, a certain
amount of data has been accessible. Although the routine laboratory
tests are usually within the normal ranges, an increase in levels
of ESR, serum calcium, ACP or ALP may be detected in certain
malignant cases. A known tumor marker, CEA, is beneficial for
diagnosis of the malignant tumor. Examination of the synovial fluid
has also been utilized as a diagnostic technique, which is of
marked importance in certain cases. Thus, it is important that
clinicians do not overlook the results of laboratory tests.
Radiographic features of primary patellar tumors are atypical of a
specific histotype. Histological examination remains the gold
standard diagnostic technique; however, in the light of the risk of
contamination, a needle biopsy is considered a reasonable
alternative. The incisional biopsy is recommended only if the
diagnosis and the radiographic features are paradoxical. Two key
points should be emphasized: i) During a needle biopsy, the joint
must not be entered; ii) during an incisional biopsy, the patella
and quadriceps tendon, the joint cavity and the synovial membrane
must not be contaminated (2).
Applying cytological techniques, identification of cells should
raise the attention of physicians, particularly when
differentiating diagnosis from inflammatory joint disease. Joint
aspiration and needle biopsy should first be attempted prior to
open biopsy. However, only the histological examination of the
specimen is a gold standard to indicate the origin of the
tumor.
The treatment approaches for patellar metastasis
include surgery, radiotherapy and chemotherapy. Surgery is the
optimal method for the majority of symptomatic patients who possess
a patellar tumor. Furthermore, according to distinct symptoms of
patients, suitable surgical options may include simple curettage
with bone grafting, excision, patellectomy, extensor mechanism
reconstruction and knee resection to above-knee amputation. In
order to avoid tumor spreading in the joint, extreme care should be
taken when curettage is performed. If the peripheral shell of
reactive bone cannot be retained according to preoperative
radiographic results, it is preferable to excise the patella. In
order to preserve motional function, the intact extensor apparatus
should be maintained or extensor structure be reconstructed. In the
place of patellectomy, cryotherapy allows anatomical preservation.
The patella-preserving surgery may achieve local remission and
preserves the patient's quality of life (8). The appropriate surgical intervention
combined with radiotherapy and chemotherapy may be rational due to
regional invasion or metastases. Radiotherapy has been used in
patellar metastases following patellectomy and extensive resection
of soft tissue. For certain postoperative tumors, radiotherapy was
deemed inappropriate as a result of radiation-induced malignant
degeneration (54). Radiotherapy was
only utilized in multiple malignant lesions, particularly
hematological and vascular malignancies (2). Neoadjuvant chemotherapy has become a
potential treatment for specific patellar malignant tumors. Of
course, attention should also be paid to the treatment of the
primary malignancies. Usually, combined therapy of multiple sites
is necessary.
Conclusion
These cases were summarized in order to highlight a
number of simple yet powerful learning points: Despite being rare,
during the differential diagnosis of a common orthopedic symptom,
anterior knee pain, one should be aware of the rare possibility
that it could be caused by patellar metastasis. More unidentified
cases of patellar metastasis may be gradually confirmed. Limited by
the knowledge of the characteristics of patellar metastasis, the
integrated diagnosis should be considered seriously. The extended
application of CT, MRI and even PET-CT is necessary. Innovative
non-invasive biopsy is required to aid specimen collection without
resulting in contamination. With improved oncological management of
patients, the functional outcome of treatment may be considered,
resulting in less debilitating surgery. On occasion, in order to
relieve the anterior knee pain and retain patient function, the
more standard and effective treatment ought to be outlined
individually. With an increasing focus on the diagnosis and
treatment of these lesions, further types of patellar metastasis
are expected to be reported in the future.
Glossary
Abbreviations
Abbreviations:
|
ESR
|
erythrocyte sedimentation rate
|
|
ACP
|
acid phosphatase
|
|
ALP
|
alkaline phosphatase
|
|
CEA
|
carcinoembryonic antigen
|
|
CRP
|
C-reactive protein
|
|
CT
|
computed tomography
|
|
MRI
|
magnetic resonance imaging
|
|
RCC
|
renal cell carcinoma
|
References
|
1
|
Unni KK: OsteosarcomaDahlin's bone tumors.
General aspects and data on 11.087 cases. Devaney K: 5th.
Lippincott-Raven Publishers; Philadelphia: pp. 143–184. 1996
|
|
2
|
Mercuri M and Casadei R: Patellar tumors.
Clin Orthop Relat Res. 389:35–46. 2001. View Article : Google Scholar
|
|
3
|
Sousa M, Melo V, Silva E and Vale J:
Patellar metastasis as the first manifestation of an adenocarcinoma
of the lung. Chest. 145:316A2014. View Article : Google Scholar
|
|
4
|
Feng H, Li H, Wang J, Zhang X and Feng J:
Squamous carcinoma of the lung metastases to the patella. Clin Nucl
Med. 40:504–505. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Pazzaglia UE, Barbieri D and Cherubino P:
Solitary metastasis of the patella as the first manifestation of
lung cancer. Int Orthop. 13:75–76. 1989. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Tudor A, Sestan B, Jonjic N, Miletic D,
Hadzisejdic I, Prpic T and Rakovac I: Solitary metastasis of the
patella in the differential diagnosis of anterior knee pain. West
Indian Med J. 59:110–112. 2010.PubMed/NCBI
|
|
7
|
Broomfield J, Ralte P, Morapudi S,
Vasireddy N and Kershaw S: Anterior knee pain: An unusual
presentation of renal cell carcinoma. J Surg Case Rep.
2014:rju0182014. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Lim CT, Wong AS, Chuah BY, Putti TC,
Stanley AJ and Nathan SS: The patella as an unusual site of renal
cell carcinoma metastasis. Singapore Med J. 48:e314–e319.
2007.PubMed/NCBI
|
|
9
|
Sun EC, Nelson SD, Seeger LL, Lane JM and
Eckardt JJ: Patellar metastasis from a squamous carcinoma of the
lung: A case report. Clin Orthop Relat Res. 391:234–238. 2001.
View Article : Google Scholar
|
|
10
|
Aktas S, Demiral H, Bilgi S, Caglar T and
Calpur OU: Patellar metastasis from a lung epidermoid carcinoma.
Yonsei Med J. 39:474–177. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Kwa S and Nade S: Metastasis in a patella:
A rare site. Aust N Z J Surg. 59:351–352. 1989. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Sur RK, Singh DP, Dhillon MS, Gupta BD,
Murali B and Sidhu R: Patellar metastasis: A rare presentation. Br
J Radiol. 65:722–724. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Wu B, Xiu Y, Jiang L and Shi H: SPECT/CT
imaging of patella metastasis from a squamous carcinoma of the
lung. Clin Nucl Med. 38:125–127. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Benedek TG: Lysis of the patella due to
metastatic carcinoma. Arthritis Rheum. 8:560–567. 1965. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Gall EP, Didizian NA and Park Y: Acute
monarticular arthritis following patellar metastasis, a
manifestation of carcinoma of the lung. Jama. 229:188–189. 1974.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Codreanu I, Zhuang H, Alavi A and Torigian
DA: Patellar metastasis from lung adenocarcinoma revealed by FDG
PET/CT. Clin Nucl Med. 37:623–624. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Ganjoo KN, Loyal JA, Cramer HM and Loehrer
PJ: Lung cancer presenting with solitary bone metastases. Case.
1:Metastatic adenocarcinoma to the patella. J Clin Oncol 17:
2995–2997. 1999.
|
|
18
|
Pauzner R, Istomin V, Segal-Lieberman G,
Matetzky S and Farfel Z: Bilateral patellar metastases as the
clinical presentation of bronchogenic adenocarcinoma. J Rheumatol.
23:939–941. 1996.PubMed/NCBI
|
|
19
|
Cooper ME and Mess D: Isolated skeletal
metastasis to the patella. Am J Orthop (Belle Mead NJ). 29:210–212.
2000.PubMed/NCBI
|
|
20
|
Rosenthal MA and Tiver KW: Patellar
metastases in the presence of chondrocal cinosis. Australas Radiol.
35:197–198. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Patel MR and Desai SS: Patellar
metastases. A case report and review of the literature. Orthop Rev.
17:687–690. 1988.PubMed/NCBI
|
|
22
|
Humphreys L and Sridhar M: Patellar
metastasis. Lancet. 359:17392002. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Meddeb N, Hamza S, Moalla M, Siala M and
Sellami S: Patelar metastasis of primary lung cancer. Rev Pneumol
Clin. 59:176–178. 2003.(In French). PubMed/NCBI
|
|
24
|
Hyde L and Hyde CI: Clinical
manifestations of lung cancer. Chest. 65:299–306. 1974. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Howlett SA and Caranasos GJ: Metastatic
renal cell carcinoma producing arteriovenous shunt. Arch Intern
Med. 125:493–495. 1970. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Doshi D, Saab M and Singh N: Atypical
presentation of renal cell carcinoma: A case report. J Med Case
Rep. 1:262007. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Warner GC, Dodds RDD and Malone PR:
Pathological fracture of the patella as the first presentation of
renal cell carcinoma. Knee. 6:281–283. 1999. View Article : Google Scholar
|
|
28
|
Nathan SS, Lim CT, Chuah BY, Putti TC,
Stanley AJ and Wong AS: Renal cell carcinoma bony metastasis
treatment. Ann Acad Med Singapore. 37:247–248. 2008.PubMed/NCBI
|
|
29
|
Keeley CD: Bilateral patellar metastases
from carcinoma of the male breast. Can J Surg. 16:328–329.
1973.PubMed/NCBI
|
|
30
|
Taylor GH: Pathologic fracture of the
patella caused by metastatic carcinoma. N Y State J Med.
64:430–431. 1964.PubMed/NCBI
|
|
31
|
Klenerman L: A Metastatic deposit in the
patella from a carcinoma of the breast. Postgrad Med J. 41:284–286.
1965. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Stoler B and Staple TW: Metastases to the
patella. Radiology. 93:853–856. 1969. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Ashby ME and Dappen N: Esophageal
carcinoma metastatic to the patella. A case report. Jama.
235:2519–2520. 1976. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Tos L and Salvi V: Tumori Della RotulaTos
L and Salvi V: La Patologia Non Traumatica Della Rotula. Torino,
Edizioni Minerva Medica; pp. 195–208. 1968
|
|
35
|
Griener B and Müller-Färber J: Patellar
metastasis of colon carcinoma. Rare occurrence in differential
diagnosis of acute knee pain: Case report. Unfallchirurg.
104:778–781. 2001.(In German).
|
|
36
|
Urvoy P, Mestdagh H, Butin E,
Lecomte-Houcke M and Maynou C: Patellar metastasis from a large
bowel adenocarcinoma. Acta Orthop Belg. 59:409–411. 1993.PubMed/NCBI
|
|
37
|
Weinert CR and Wiss DA: Unusual lesions of
the patella. Orthopedics. 2:378–383. 1979.PubMed/NCBI
|
|
38
|
Boyd HB and Hawkins BL: Patellectomy; a
simplified technique. Surg Gynecol Obstet. 86:3571948.PubMed/NCBI
|
|
39
|
Jaeger HJ, Kruegener GH and Donovan AG:
Patellar metastasis from a malignant melanoma. Int Orthop.
16:282–284. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Tas F and Keskin S: Patellar metastasis of
melanoma. Indian J Med Res. 138:3702013.PubMed/NCBI
|
|
41
|
Cole WH: Primary tumors of the patella. J
Bone Joint Surg. 23:637–654. 1925.
|
|
42
|
Ehara S, Khurana JS, Kattapuram SV,
el-Khoury GY and Rosenthal DI: Osteolytic lesions of the patella.
AJR Am J Roentgenol. 153:103–106. 1989. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Sutro CJ: Lymphosarcoma of the patella:
Radical excision without repair of the extensor apparatus of the
leg. Bull Hosp Joint Dis. 24:68–74. 1963.PubMed/NCBI
|
|
44
|
Choi YS, Yoon YK, Kwak HY and Song IS:
Patellar metastasis from squamous cell carcinoma of the larynx. AJR
Am J Roentgenol. 174:1794–1795. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Singh HK, Silverman JF, Ballance WA Jr and
Park HK: Unusual small bone metastases from epithelial
malignancies: Diagnosis by fine-needle aspiration cytology with
histologic confirmation. Diagn Cytopathol. 13:192–625. 1995.
View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Kawamura H, Ogata K, Miura H and Sugioka
Y: Patellar metastases: A report of two cases. Int Orthop.
17:57–59. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Song M, Zhang Z, Wu Y, Ma K and Lu M:
Primary tumors of the patella: World. J Surg Oncol. 13:1632015.
|
|
48
|
Scapinelli R: Blood supply of the human
patella. Its relation to ischaemic necrosis after fracture. J Bone
Joint Surg Br. 49:563–570. 1967.PubMed/NCBI
|
|
49
|
Sosnoski DM, Norgard RJ, Grove CD, Foster
SJ and Mastro AM: Dormancy and growth of metastatic breast cancer
cells in a bone-like microenvironment. Clin Exp Metastasis.
32:335–344. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Fearon ER and Vogelstein B: A genetic
model for colorectal tumorigenesis. Cell. 61:759–767. 1990.
View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Bessa X, Elizalde JI, Boix L, Piñol V,
Lacy AM, Saló J, Piqué JM and Castells A: Lack of prognostic
influence of circulating tumor cells in peripheral blood of
patients with colorectal cancer. Gastroenterology. 120:1084–1092.
2001. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Kang Y: Breast cancer bone metastasis:
Molecular basis of tissue tropism. J Musculoskelet Neuronal
Interact. 4:379–380. 2004.PubMed/NCBI
|
|
53
|
Ferguson PC, Griffin AM and Bell RS:
Primary patellar tumors. Clin Orthop Relat Res. 336:199–204. 1997.
View Article : Google Scholar
|
|
54
|
Okada K, Sato K, Abe E, Kataoka Y,
Miyakoshi N, Ishikawa N and Sageshima M: Case report 858:
Postradiation osteosarcoma of the patella. Skeletal Radiol.
23:471–474. 1994. View Article : Google Scholar : PubMed/NCBI
|