Introduction
A solitary fibrous tumour (SFT) is a rare,
slow-growing, mesenchymal neoplasm arising from the pleura, which
is unrelated to asbestos exposure or cigarette smoking (1) and was initially described in 1931
(2). Over the past 80 years, SFTs
have been identified in numerous extrapleural locations, including
the nasal cavity (3), breast
(4), stomach (5), bronchus (6), head and neck (7), liver (8),
oesophagus (9), pelvic (10), pancreas (11), prostate (12), orbit (13), central nervous system (14), parotid gland (15), kidney (16), lung (17), sella turcica (18), heart (19), conus medullaris (20), omentum (21), infratemporal fossa (22), bladder (23), soft tissues of the extremities
(24), palatine tonsil (25), diaphragm (26), mesentery (27), lumbar spine (28), thymus (29), oral cavity (30), spermatic cord (31), thyroid (32), rectum (33), salivary glands (34), retroperitoneum (35), larynx (36), trachea (37), adrenal gland (38), female genital tract (39), periosteum of bone (40), mediastinum (41) and hypopharynx (42).
To our knowledge, SFTs are extremely rare in the
lung (43). There are few detailed
case reports concerning the clinical course, imaging
characteristics, diagnosis, treatment and prognosis of primary
intrapulmonary SFTs. The main purpose of the present study was to
report our experience with the diagnosis and management of primary
intrapulmonary SFTs and to systematically review previously
reported cases in the literature.
Patients and methods
We retrospectively reviewed the records of 5
patients with primary intrapulmonary SFTs who underwent surgical
resection at the Department of Cardiothoracic Surgery, Lishui
Center Hospital (Lishui, China), and Clinical College of Yangzhou
University, (Yangzhou, China), between January 2000 and January
2016. Age, sex, medical history, clinical presentation, diagnostic
methods, intraoperative findings, postoperative complications and
outcome were retrieved from hospital records. Meanwhile, relevant
studies regarding intrapulmonary SFTs were searched via PubMed from
January 1990 to January 2016. The text words and MeSH terms
‘Solitary fibrous tumours’, ‘Intrapulmonary’, and ‘Lung’ were used.
Tumour characteristics, clinicopathologic features, therapeutic
strategy and survival outcomes were reviewed, and these data were
tabulated.
Results
Report of cases
Of the five cases, all were males, with a mean age
of 57.6 years (range, 37–68 years). Two patients (nos. 2 and 5) had
history of hypertensive disease. One patient (no. 2) had history of
diabetes mellitus. One patient (no. 1) had history of bronchial
asthma. One patient (no. 3) had history of nodular goitre. The
remaining patient (no. 4) had no history of any disease. All
patients were asymptomatic, and their tumours were discovered
incidentally on routine computed tomography (CT) examination.
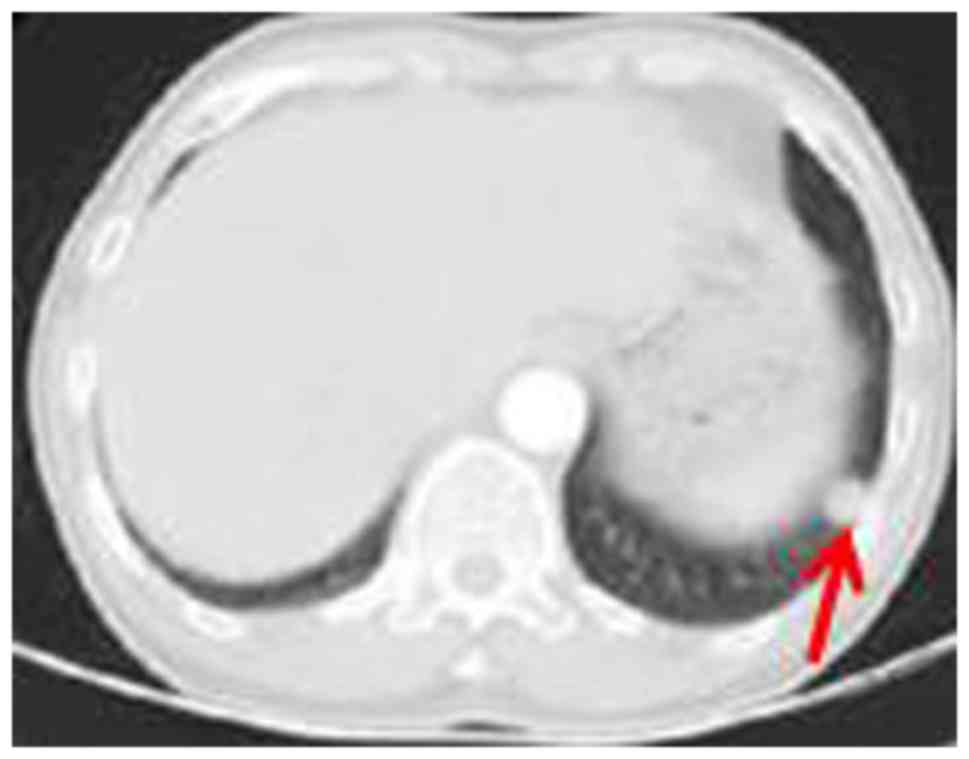
Contrast-enhanced CT of the chest revealed a lung mass with no
calcification or any fatty tissue (Fig.
1). One, one, one and two tumours occurred in the right lower,
left upper, right upper and left lower lung, respectively. Three
patients (nos. 1–3) were preoperatively diagnosed with spindle cell
tumour by CT-guided percutaneous aspiration biopsy. Other
examinations, including pulmonary function, echocardiogram,
electrocardiogram, coagulation function and blood routine
examination, were normal. The serum levels of Na+,
K+, Cl−, Ca2+, Mg2+
were all within reference range. Serum carbohydrate antigen,
carcino-embryonic antigen, squamous cell antigen and
neuron-specific enolase were within normal limits. No evidence of
metastasis was found via head magnetic resonance imaging (MRI) and
abdominal ultrasound.
One patient underwent tumour enucleation though
thoracotomy (no. 1), one patient underwent upper left lobectomy
associated with lymph node dissection involving radical dissection
of the mediastinum (no. 2), and one patient underwent tumour
resection associated with bilateral subtotal thyroidectomy (no. 3).
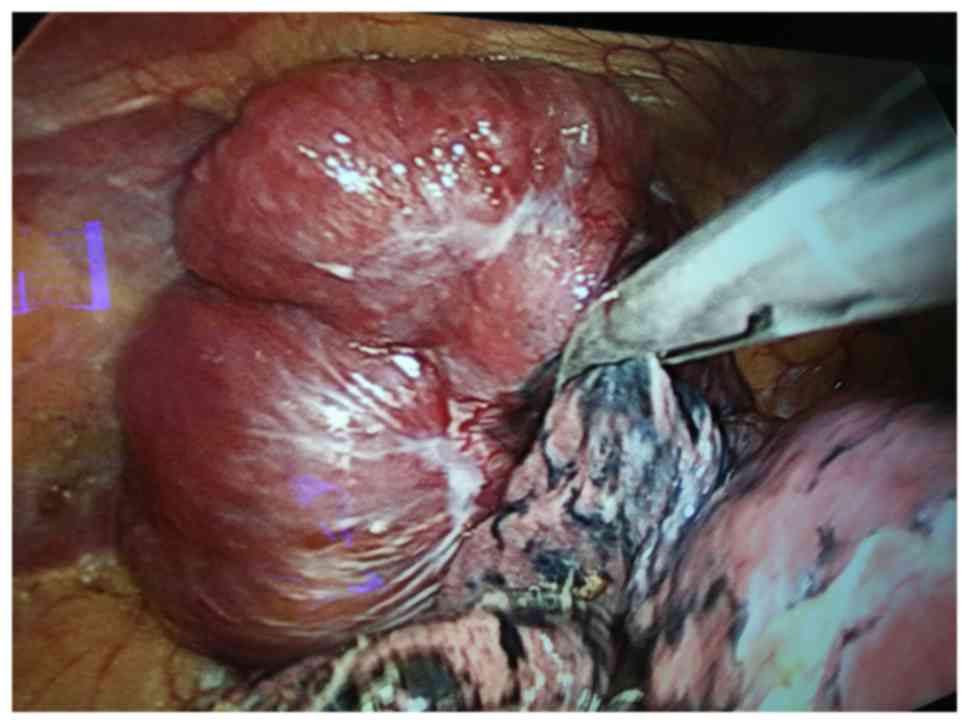
The remaining two patients underwent tumour enucleation via
video-assisted thoracoscopic surgery (VATS) (nos. 4 and 5)
(Figs. 2 and 3). Data of the clinical features are shown
in Table I.
 | Table I.Patient characteristics and treatment
history in our study. |
Table I.
Patient characteristics and treatment
history in our study.
| Features | Patient no. 1 | Patient no. 2 | Patient no. 3 | Patient no.4 | Patient no.5 |
|---|
| Sex | Male | Male | Male | Male | Male |
| Age (years) | 37 | 59 | 59 | 65 | 68 |
| Presentation | Asymptomatic | Asymptomatic | Asymptomatic | Asymptomatic | Asymptomatic |
| Previous
history | Bronchial
asthma | hypertensive
disease, diabetes mellitus | Nodular goiter | No | hypertensive
disease |
| Paraneoplastic
syndrome | No | No | No | No | No |
| Location of
lesions | Right lower
lobe | left lower
lobe | Left upper
lobe | left lower
lobe | Right upper
lobe |
| Surgical
strategy | Thoracotomy | Thoracotomy | Thoracotomy +
bilateral subtotal thyroidectomy | VATS | VATS |
| Surgical
procedures | Adequate wedge
resection | Left lower
lobectomy associated with lymph node dissection | Left upper
lobectomy | Adequate wedge
resection | Adequate wedge
resection |
| Operating time
(min) | 100 | 120 | 150 | 75 | 35 |
| Blood loss
(ml) | 200 | 300 | 100 | 5 | 50 |
| Size of lesion
(cm) | 2.5×3.0 | 7×5 | 6.5×3 | 1.5×1.5 | 4×3 |
| Postoperative
complication | Postoperative
hemorrhage | no | No | No | no |
| Hospital stay
(days) | 22 | 18 | 22 | 4 | 9 |
| Time of
intrathoracic drain (days) | 9 | 5 | 1 | 1 | 2 |
| Cellular
pattern | Spindle | Spindle | Spindle | Spindle | Spindle |
| Mitotic count | <1/10HPF | >10/10HPF | <5/10HPF | <1/10HPF | <5/10HPF |
| CD34 | + | + | + | + | + |
| CD99 | − | + | + | + | + |
| Bcl-2 | + | + | + | + | + |
| Vimentin | − | − | − | + | + |
| Desmin | − | − | − | − | − |
| S-100 | − | − | − | − | − |
| SMA | − | − | − | − | − |
| Diagnosis | Benign | Malignant | Benign | Benign | Benign |
| Follow up
(months) | 38 | 67 | 55 | 27 | 1 |
| Recurrence | Unknown | No | No | No | No |
| Present status | Unknown | NED | NED | NED | NED |
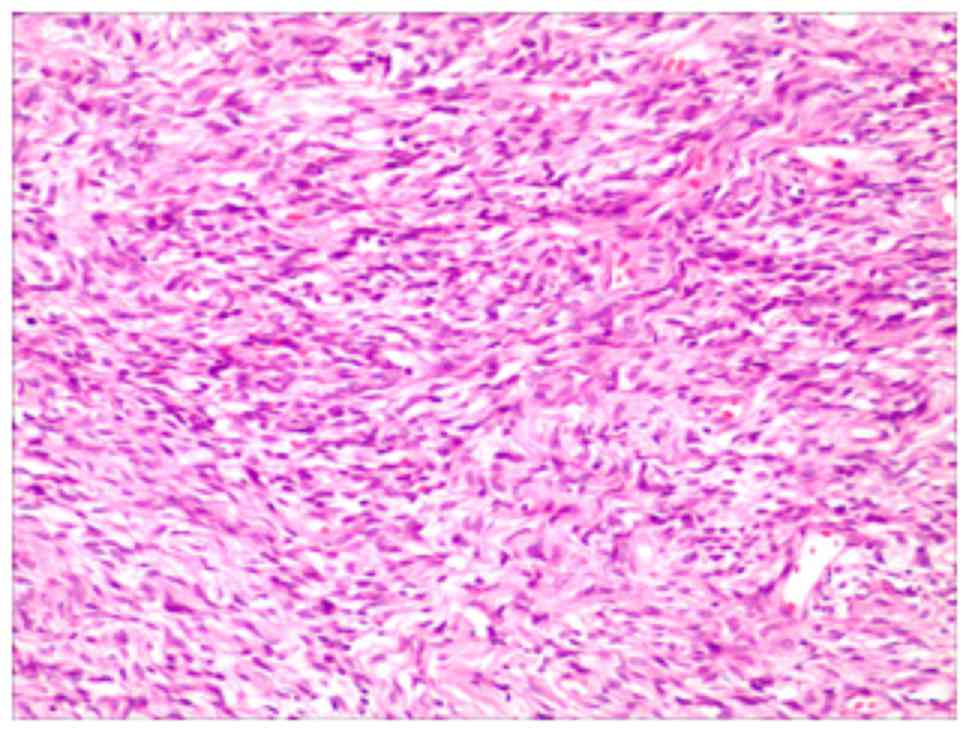
The haematoxylin and eosin (H&E) stain showed a
rich variety of spindle cells and amorphous areas of collagen
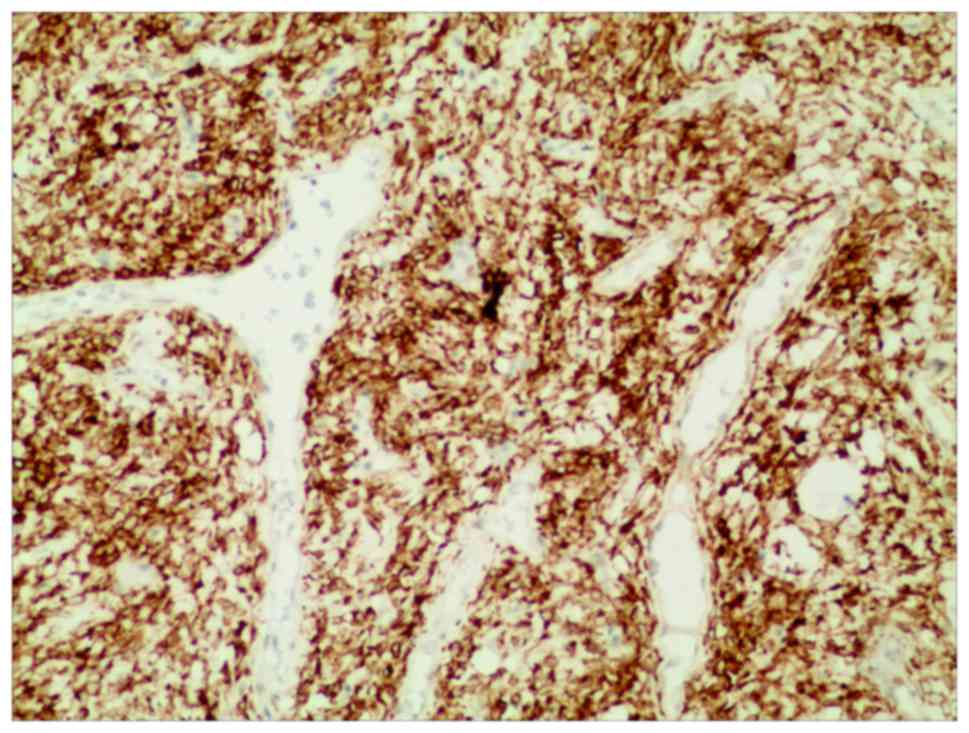
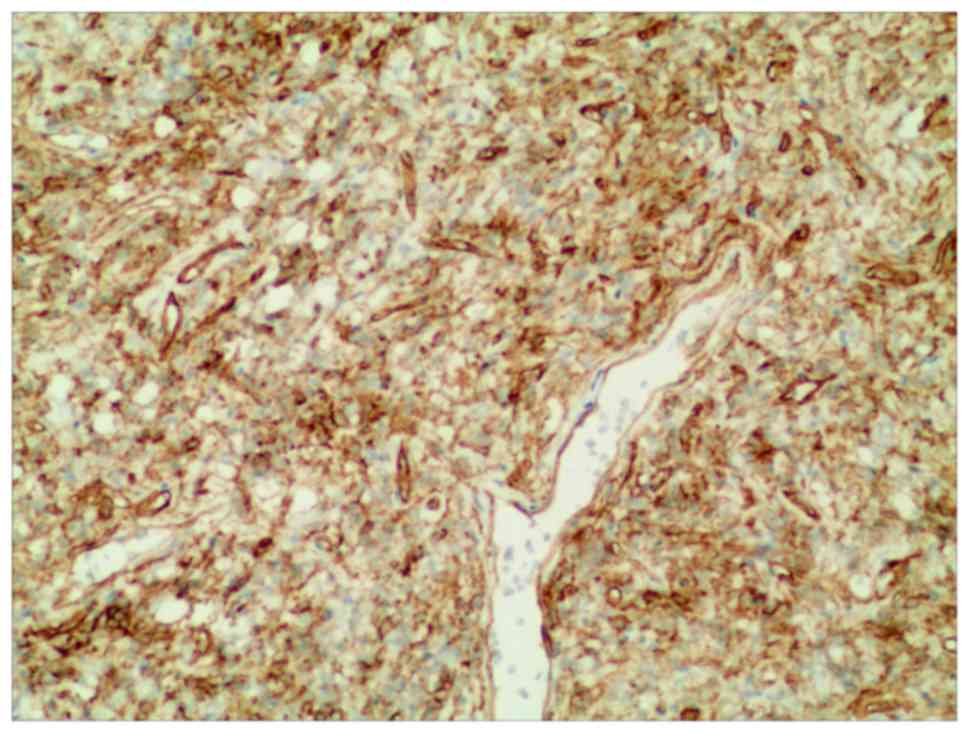
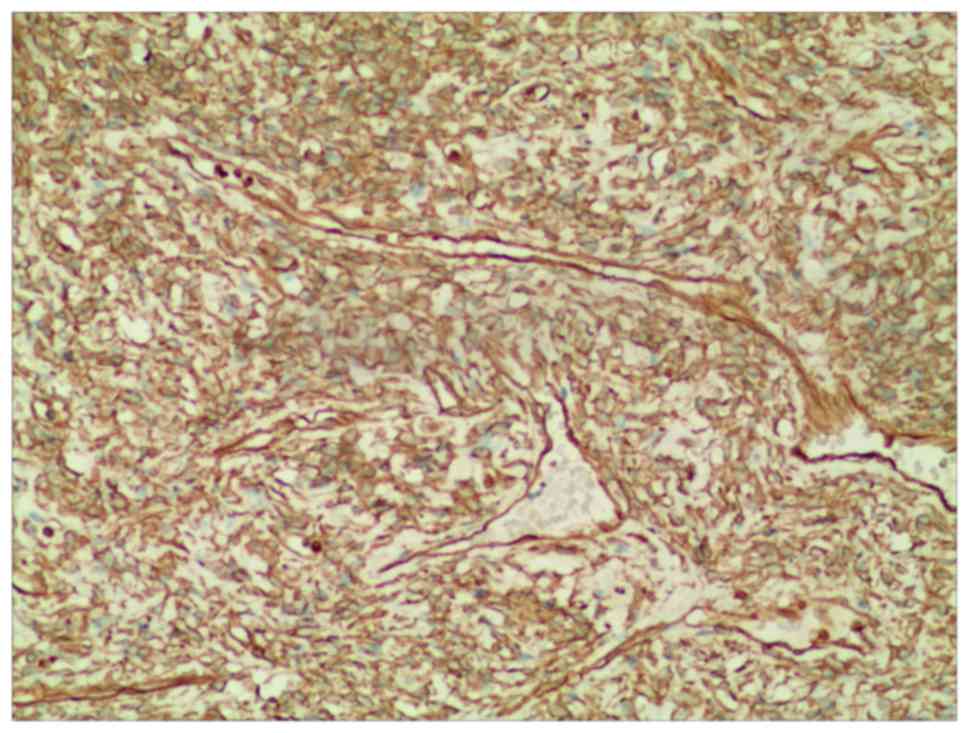
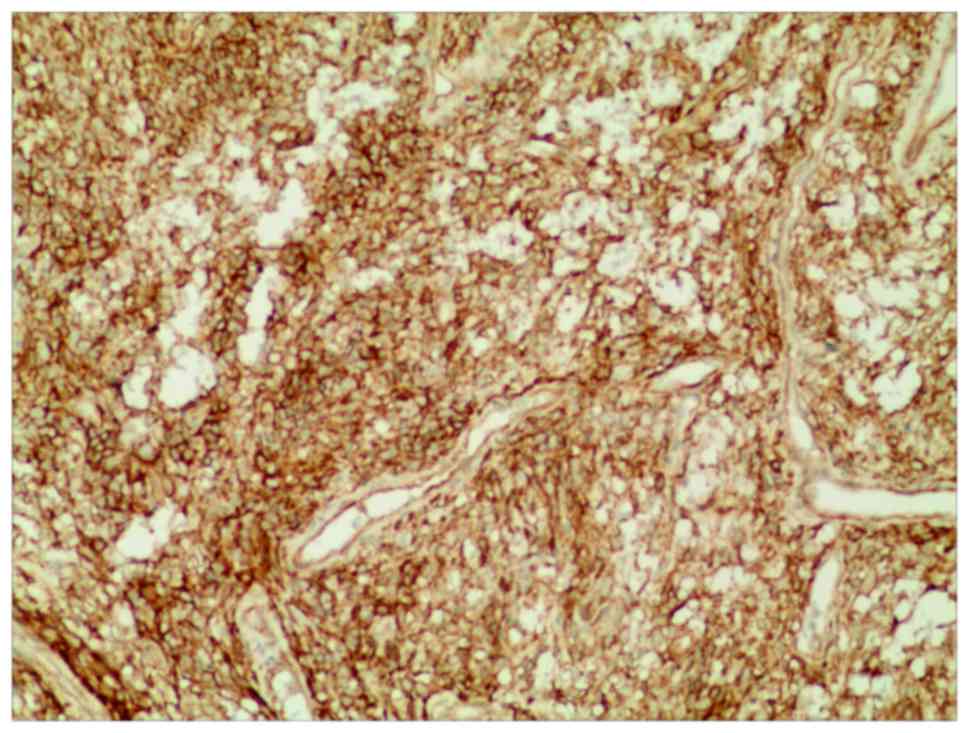
(Fig. 4). Immunohistochemical
reactions of the tumour cells were strongly positive for B-cell
lymphoma (Bcl)-2 (Fig. 5) and cluster
of differentiation (CD)34 (Fig. 6).
Tumour cells were positive for vimentin (nos. 4 and 5) (Fig. 7) and CD99 (nos. 2–5) (Fig. 8). The tumour cells were negative for
CD117, desmin, smooth muscle actin (SMA), epithelial membrane
antigen and S-100. Following an immunohistochemical-analysis-based
study, the diagnosis of intrapulmonary SFTs was made.
Postoperative haemorrhage occurred in one patient
(no. 1), and he received surgical intervention for haemostasis. The
average time of intrathoracic drain was 3.6 (1–9) days. The
average hospital stay was 15 (4–22) days,
and no mortality occurred. All patients were discharged from the
hospital following an uneventfully recovery. The mean length of the
postoperative follow-up was 37.6 (1–67) months.
One patient was lost to follow-up, and four patients were
asymptomatic.
Published case study findings
Nineteen articles were identified from the searches
of databases (17,43–59)
(Table II). They had a total of 45
patients: Twenty-three males and 22 females. The mean age was 59.4
years, ranging from 7 to 81 years. Twelve patients were
asymptomatic, and pain and cough were the major symptoms. Five,
one, two, four, and seventeen tumours occurred in the right upper
lobe, right middle lobe, right lower lobe, left upper lobe and left
lower lobe, respectively. Thirty-nine patients underwent surgery,
one patient underwent radiotherapy, and one patient underwent
radiofrequency ablation. Twenty-two patients were followed up, and
the mean length of the postoperative follow-up was 48 (1–168)
months. One patient was diagnosed with chest wall metastases. Five
patients died (Table III).
| Table II.Clinicopathologic features of
intrapulmonary solitary fibrous tumours present in the English
literature. |
Table II.
Clinicopathologic features of
intrapulmonary solitary fibrous tumours present in the English
literature.
| Authors (ref.) | Case | Age (years) | Sex | Site | Size | Symptoms | Treatment | Follow-up
(months) | Status |
|---|
| Cardinal et
al (43) | 3 | 44 | Male | Left lower
lobe | 4 cm | Chest
discomfort | Segmental
resection | 48 | NED |
|
|
| 64 | Male | Left lower
lobe | 6 cm | asymptomatic | Left lower
lobectomy | 36 | NED |
|
|
| 47 | Male | Left lower
lobe | 3 cm | Asymptomatic | Tumor
resection | 12 | NED |
| Ikeda et al
(44) | 1 | 80 | Female | Left lower
lobe | Unknown | Back pain | Radiotherapy | 11 | Died |
| Sironi et al
(45) | 1 | 68 | Male | Left lower
lobe | 8.8×5.7×5 cm | Asymptomatic | Unknown | Unknown | Unknown |
| Dong et al
(46) | 1 | 18 | Male | Bilateral
lungs | Unknown | asymptomatic | Unknown | Unknown | Unknown |
| van de Rijn et
al (47) | 2 | 69 | Male | Unknown | 12 cm | Unknown | Autopsy | No | Died |
|
|
| 80 | Female | Unknown | Unknown | Unknown | Unknown | 79 | NED |
| Demırağ et
al (48) | 1 | 56 | Female | Left lung | 16 cm | Unknown | Left
pneumonectomy | 87 | Unknown |
| Barrettara et
al (49) | 1 | 81 | Female | Left lower
lobe | 10×9 cm | Left thoracic
pain | Left inferior
lobectomy | Unknown | Unknown |
| Patsios et
al (50) | 1 | 50 | Male | Left lower
lobe | 2.7 cm | Asymptomatic | Wedge
resection | Unknown | Unknown |
| Sakurai et
al (51) | 1 | 40 | Male | Left lower
lobe | 2.2 cm | Asymptomatic | Wedge
resection | 14 | NED |
| Sagawa et al
(52) | 1 | 72 | Female | Left upper
lobe | 12×9×7 mm | Asymptomatic | Wedge
resection | 12 | NED |
| Geramizadeh et
al (53) | 1 | 7 | Male | Right upper
lobe | 5 cm | Cough and
dyspnea | Right
pneumonectomy | 9 | NED |
| Kawaguchi et
al (17) | 1 | 60 | Female | Left upper
lobe | 23×22×19 mm | Asymptomatic | Left upper
segmentectomy | 6 | NED |
| Rao et al
(54) | 24 | 83 | Male | Right lung | 13.0 cm | Unknown | Wedge excision or
lobectomy | <60 | NED |
|
|
| 75 | Female | Unknown | Unknown |
|
| <60 | NED |
|
|
| 73 | Female | Left lower
lobe | 2.3 cm |
|
| <60 | NED |
|
|
| 69 | Male | Left lower
lobe | Unknown |
|
| <60 | NED |
|
|
| 59 | Female | Unknown | Unknown |
|
| <60 | NED |
|
|
| 52 | Female | Left upper
lobe | 2.5 cm |
|
| 108 | NED |
|
|
| 49 | Male | Unknown | 18.0 cm |
|
| 168 | NED |
|
|
| 58 | Female | Left lower
lobe | 3.9 cm |
|
| <60 | NED |
|
|
| 46 | Male | Right lung | 4.5 cm |
|
| 156 | NED |
|
|
| 64 | Male | Right upper
lobe | 5.0 cm |
|
| 84 | Died |
|
|
| 68 | Female | Left lung | Unknown |
|
| Unknown | Unknown |
|
|
| 60 | Male | Left lower
lobe | Unknown |
|
| Unknown | Unknown |
|
|
| 59 | Male | Right upper
lobe | Unknown |
|
| Unknown | Unknown |
|
|
| 44 | Female | Right upper
lobe | Unknown |
|
| Unknown | Unknown |
|
|
| 50 | Female | Left lower
lobe | Unknown |
|
| Unknown | Unknown |
|
|
| 81 | Female | Unknown | 7.0 cm |
|
| Unknown | Unknown |
|
|
| 61 | Male | Right lower
lobe | 22.0 cm |
|
| 48 | Died |
|
|
| 64 | Female | Left lower
lobe | 12.0 cm |
|
| <60 | NED |
|
|
| 62 | Male | Unknown | 8.0 cm |
|
| <60 | NED |
|
|
| 44 | Female | Left lung | 4.5 cm |
|
| <60 | NED |
|
|
| 73 | Female | Unknown | 3.5 cm |
|
| <60 | NED |
|
|
| 75 | Female | Unknown | 10.0 cm |
|
| 60 | Chest wall |
|
|
|
|
|
|
|
|
|
| metastases |
|
|
| 59 | Female | Left lung | 10.0 cm |
|
| Unknown | Unknown |
|
|
| 45 | Male | Left lower
lobe | 3.0 cm |
|
| 60 | Died |
| Caruso et al
(55) | 1 | 72 | Male | Left lower
lobe | 6.0 cm | Asymptomatic | Left lower
lobectomy | 12 | NED |
| Fridlington et
al (56) | 1 | 56 | Male | Left lower
lobe | 20 cm | Symptomatic
hypoglycemia | Pneumonectomy | 1 | NED |
| Kouki et al
(57) | 1 | 52 | Male | Right upper
lobe | 5.3×5.0 cm | Asymptomatic | Right upper
lobectomy | 24 | NED |
| Baliga et al
(58) | 1 | 42 | Male | Right lower
lobe | 11 cm | Asymptomatic | Radiofrequency
ablation | No | Died |
| Khalifa et
al (59) | 1 | 71 | Female | Right middle
lobe | 2.8 cm | Presistent cough
with clear sputum | Wedge lung
resection | 10 | NED |
| Chang et al
(60) | 1 | 73 | Female | Left lower
lobe | 3×3×2 cm | Asymptomatic | Lobectomy | 12 | NED |
| Table III.Characteristics of the primary
intrapulmonary solitary fibrous tumors present in the English
literature. |
Table III.
Characteristics of the primary
intrapulmonary solitary fibrous tumors present in the English
literature.
| No. of studies | 19 |
|---|
| No. cases | 45 |
| Age (years) |
|
|
Mean | 59.4 |
|
Range | 7–81 |
| Tumor sizes
(cm) |
|
|
Mean | 8.2 |
|
Range | 2–23 |
| Sex |
|
|
Male | 23 (51.1%) |
|
Female | 22 (48.9%) |
| Symptoms | 18 |
|
Asymptomatic | 12 (66.7%) |
|
Pain | 2 (11.1%) |
|
Cough | 2 (11.1%) |
|
Other | 2 (11.1%) |
| Localization | 29 |
| Right
upper lobe | 5 (17.2%) |
| Right
middle lobe | 1 (3.5%) |
| Right
lower lobe | 2 (6.9%) |
| Left
upper lobe | 4 (13.8%) |
| Left
lower lobe | 17 (58.6%) |
| Treatment | 41 |
|
Surgery | 39 (95.2%) |
|
Radiotherapy | 1 (2.4%) |
|
Radiofrequency ablation | 1 (2.4%) |
Pathologic and immunohistochemical
features
Twenty-eight of 32 cases showed low mitotic counts
(0–5/10 HPF), 1 of 32 had a middle mitotic count (0–6/10 HPF), and
3 of 32 showed high mitotic counts (5–10/10 HPF).
Immunohistochemical staining analyses were performed in 28 cases.
Twenty-four of 28 cases were CD34-positive. Ten of 13 cases were
CD99-positive. Fourteen of 15 cases were Bcl-2 positive. Fourteen
of 16 cases were vimentin positive. Five of 17 cases were smooth
muscle antibody (SMA)-positive. Two of 9 cases were epithelial
membrane antigen (EMA) positive. Eight of 9 cases were
mib-monoclonal antibody-1 (MIB-1)-positive (Table IV).
| Table IV.Pathologic and immunohistochemical
features presented in the English literature. |
Table IV.
Pathologic and immunohistochemical
features presented in the English literature.
| Author | Mitotic count |
Immunohistochemistry |
|---|
| Sironi et al
(45) | NA | CD34+,
CD99+ |
| Dong et al
(46) | NA |
Vimentin+, CD34+,
EMA−, CAM5.2-, S-100−, SMA-,
desmin−, HMB45- |
| van de Rijn et
al (47) | NA | CD34+,
SMA-, MSA−, desmin-, AE1−, CAM5- |
| Demırağ et
al (48) | 2/10 HPF | CD44+++,
MMP-2+ |
| Barrettara et
al (49) | 2/10 HPF | CD34+,
CD99+, Bcl-2+, vimentin+, calretinin−, S100-,
actine−, CK- |
| Patsios et
al (50) | NA |
Vimentin+, CD34: focal+,
CK−, S-100-, SMA− |
| Sakurai et
al (51) | NA | Vimentin+,
CD34+, Bcl-2+, CK−, desmin-, SMA−,
S-100- |
| Sagawa et al
(52) | Rare | CD34+,
TTF-1-, MIB-1− |
| Geramizadeh et
al (53) | 0/10 HPF | Vimentin+,
CD34+, Bcl-2+, CK−, desmin-, SMA−,
S-100- |
| Kawaguchi et
al (17) | NA | CD34+,
calretinin-, SMA−, S-100- |
| Rao et al
(54) | 2-5/10 HPF | NA |
|
| 2-5/10 HPF |
Vimentin+, p53+,
Bcl-2+, CD34+, CD99+, MIB-1++, CK
AE1/AE3−, EMA-, S100−, SMMS-1- |
|
| <1/10 HPF | NA |
|
| <1/10 HPF | NA |
|
| <1/10 HPF | NA |
|
| <1/10 HPF | NA |
|
| 2-5/10 HPF | Bcl-2+,
CD34+, CD99+, MIB-1+, SMA+, vimentin-,
p53−, calponin-, AE1/3−, EMA-,
S100−, SMMS1- |
|
| <1/10 HPF | Bcl-2+,
CD34+, CK AE1/3−, SMA- |
|
| 2-5/10 HPF | NA |
|
| <1/10 HPF | CD34+,
CD99+, MIB-1+, SMA-, CK AE1/3− |
|
| <1/10 HPF | NA |
|
| 2-5/10 HPF | NA |
|
| <1/10 HPF | NA |
|
| <1/10 HPF | NA |
|
| <1/10 HPF | NA |
|
| <1/10 HPF | NA |
|
| 2-5/10 HPF | Vimentin+++,
Bcl-2+++, calponin++, CD34++, CD99-weak+, CK
AE1/3: focal+, EMA-, MIB-1+, SMA- |
|
| <1/10 HPF |
Bcl-2+++, CD34+,
CD99+, MIB-1+, SMA+, CK AE1/3-,
vimentin−, calponin-, EMA−, |
|
| 2-5/10 HPF | Vimentin+++,
Bcl-2+++, CD34+++, MIB-1++, CD99++,
calponin+, CK AE1/3-, EMA−, S100-,
SMA−, SMMS1- |
|
| <1/10 HPF | CD99+++,
Bcl-2+++, CD34+, p53+, MIB-1+, calponin-,
AE1/3−, EMA-, S100−, SMMS1- |
|
| <1/10 HPF | CD99−,
Bcl-2+++, CD34++, p53+, AE1/3−, SMA-,
vimentin+++, SMMS1- |
|
| 5-10/10 HPF | Bcl-2+,
CD34+, CD99+, SMA+, CK AE1/3− |
|
| >10/10 HPF | Vimentin+,
Bcl-2+, CD99+, p53−, calponin-,
CD34−, CK AE1/3-, S100−, SMA-,
SMMS1− |
|
| >10/10 HPF | MIB-1+++,
SMA++, EMA+, p53−, Bcl-2-,
calponin−, CD34-, CD99−, CK AE1/3-,
S100−, SMMS1- |
| Caruso et al
(55) | 0-6/10 HPF |
Vimentin+, keratin-,
CEA−, EMA+, F VIII−, S-100-,
desmin−, actin- |
| Fridlington et
al (56) | 1-2/10 HPF | CD34+,
vimentin+, S-100− |
| Kouki et al
(57) | 3-4/10 HPF | CD34+ |
| Baliga et al
(58) | 0/10 HPF | CD34++,
Bcl-2+, SMA+, CD99-, CAM 5.2−,
calretinin- |
| Khalifa et
al (59) | NA | CD34+,
vimentin+, S-100-, CK−, F VIII-, MSA−,
SMA- |
| Chang et al
(60) | NA | CD34+,
vimentin+, S-100−, desmin-, CEA−, a1-ACT-, F
VIII− |
Discussion
SFTs are rare, mesenchymal neoplasms initially
described in the pleura but have since been discovered in nearly
every anatomic location (61).
Klemperer and Rabin (62) reported 5
cases of primary pleural neoplasms in 1931 and proposed that SFT
was of submesothelial origin. However, in the subsequent decades,
on the basis of immunohistochemical analyses and ultrastructural
features, it is now recognized that SFTs arise from primitive
fibroblast-like cells in connective tissue (61). SFTs, to our knowledge, most often
occur in the pleura. They can be rarely found in the lung, central
nervous system, kidney and other extrapleural sites. Via searches
of databases, a total of 45 patients with intrapulmonary SFTs were
found.
Intrapulmonary SFTs are usually found incidentally
and may be associated with chest pain and cough. Seventeen patients
(5 in our study and 12 in published literature) were asymptomatic
and were discovered incidentally. Two patients presented with pain,
and two patients presented with cough. Of note, few patients with
SFTs present with refractory hypoglycaemia, which is a
paraneoplastic syndrome that secretes a prohormone form of
insulin-like growth factor-II (IGF-II), referred to as the
Doege-Potter syndrome (DPS).
Due to their atypical clinical and radiographic
appearance as a common lung tumour, the diagnosis of intrapulmonary
SFTs presents unique challenges. Imaging examinations, including
chest X-rays, CT and MRI, are used for assessing intrapulmonary
SFTs. There are limited data on X-rays and CT imaging features of
intrapulmonary SFTs. The available data show that intrapulmonary
SFTs are well-defined ovoid or round pulmonary nodules on chest
X-rays and CT scanning, but they are non-specific. The PET-CT
findings of SFTs have been rarely reported. PET-CT is a useful tool
for evaluating the size, regional invasion and distant metastasis
of a tumour. Yan et al (63)
have reported a malignant SFT with mildly increased FDG uptake.
Dong et al (46) have reported
a benign SFT with intense FDG uptake. The clinical behaviour of the
tumour may be predicted based on PET-CT findings, and FDG uptake
degree may be related to the tumour's aggressive behaviour
(46). An intrapulmonary SFT may be
identified by CT-guided percutaneous aspiration biopsy. Caruso
et al (55) operated on a
pulmonary mass CT-guided FNA cytology biopsy. The FNA cytologic
specimen contained spindle cells. Furthermore, FNA cytology, proper
clinical and radiologic findings are helpful in narrowing the
diagnostic possibilities and making tentative pathologic diagnoses.
However, spindle-shaped cells also appear in fibrosarcoma,
leiomyosarcoma, schwannoma and others. Therefore, the diagnosis of
SFTs may not be identified without immunohistochemical staining.
The differential diagnosis of intrapulmonary SFT includes numerous
malignant and benign tumours, including pulmonary adenofibroma,
benign neural neoplasms, leiomyoma, leiomyosarcoma, synovial
sarcoma, spindle cell thymoma, spindle cell carcinoid tumour, nerve
sheath tumour, fibrosarcoma, sarcomatoid carcinoma, and sarcomatoid
mesothelioma (54). To our knowledge,
positive CD34, CD99, vimentin and Bcl-2 expression are important
markers for the diagnosis of an SFT.
Our review of previously reported cases in the
literature suggests complete surgical resection is generally
accepted as the definitive and effective treatment of choice for
intrapulmonary SFTs. Adequate wedge resection, anatomic
segmentectomy and lobectomy, according to the location of mass, are
common surgical procedures for resection of intrapulmonary tumours.
In our study, three patients underwent adequate wedge resection,
whereas the other two patients under anatomic lobectomy. In recent
decades, with the development of minimally invasive technology,
surgical approaches have been radically changed. More and more
intrapulmonary tumours can be safely and availably excised via
VATS. In our study, two patients underwent VATS. Previous studies
have used radiotherapy and radiofrequency ablation for
intrapulmonary SFTs. However, these treatments carry a higher risk
of death during follow-up. The effectiveness and capability of such
treatment has yet to be confirmed.
Due to their deficiency of information and their
languages of publication (not English), some studies were not
included in our study. Thirty-six of 681 cases and 8 of 88 cases
were SFTs of the lung and pleura, respectively, in Choi's et
al (64) and Schirosi's et
al (65) studies, and these were
not included. Gonullu et al (66) reported a case of metastatic breast
carcinoma to SFT in the lung, and Strickland et al (67) reported a case of SFT of the uterus
presenting with lung metastases. Míguez González et al
(68) reported a case of
intrapulmonary SFT associated with haemoptysis, and Masuda et
al (69) report two cases of
intrapulmonary tumours with different growth patterns. However, the
articles were not written in English. Radulescu et al
(70) reported a case of malignant
primary intrapulmonary SFT with haemangiopericytoma-like
features.
In conclusion, we retrospectively reviewed the
records of 5 patients with primary intrapulmonary SFTs who
underwent surgical resection, and we systematically reviewed
previously reported cases in the literature. This study has 4
important findings. First, intrapulmonary SFTs can occur in people
of all ages and with no sex predominance. The male-to-female ratio
was 1.0:0.96. Second, intrapulmonary SFTs are often discovered
incidentally. When symptomatic, the common symptoms are chest pain
and cough. Third, the left lower lobe was the most common site
location. Finally, complete surgical resection is a safe, effective
and successful treatment.
References
|
1
|
Rosado-de-Christenson ML, Abbott GF,
McAdams HP, Franks TJ and Galvin JR: From the archives of the AFIP:
Localizedfibrous tumorsof the pleura. Radiographics. 23:759–783.
2003. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Hanau CA and Miettinen M: Solitary fibrous
tumor: Histological and immunehistochemical spectrum of benign and
malignant variants presenting at different sites. Hum Pathol.
26:440–449. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Mathew GA, Ashish G, Tyagi AK,
Chandrashekharan R and Paul RR: Solitary fibrous tumor of nasal
cavity: A case report. Iran J Otorhinolaryngol. 27:307–312.
2015.PubMed/NCBI
|
|
4
|
Rhee SJ, Ryu JK, Han SA and Won KY:
Solitary fibrous tumor of the breast: A case report and review of
the literature. J Med Ultrason (2001). 43:125–128. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Bosković T, Zivojinov M, Sabo JI, Budakov
Z, Veljković R and Zivojinov S: Rare solitary fibrous tumor of the
stomach: A case report. Vojnosanit Pregl. 72:1035–1038. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Huang W, Xu X, Hu J, Cheng G and Xie P:
Primary solitary fibrous tumor of the bronchus: A case report. Int
J Clin Exp Pathol. 8:13596–13600. 2015.PubMed/NCBI
|
|
7
|
Fu S, Tian Z, Zhang C and He Y: Monosotic
fibrous dysplasia and solitary intramuscular myxoma of the head and
neck: A unique presentation of Mazabraud's syndrome and a
literature review. Oncol Lett. 10:3087–3094. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Silvanto A, Karanjia ND and Bagwan IN:
Primary hepatic solitary fibrous tumor with histologically benign
and malignant areas. Hepatobiliary Pancreat Dis Int. 14:665–668.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Zhu XS, Dai YC and Chen ZX: Giant solitary
fibrous tumor of esophagus resected by endoscopic submucosal
dissection. Ann Thorac Surg. 100:2340–2343. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Gao C, Zhang Y, Li YY, Yu YH, Qu W, Gao YS
and Zhang S: Postoperative recurrence solitary fibrous tumor of the
pelvic with malignant transformation. Int J Clin Exp Med.
8:16827–16833. 2015.PubMed/NCBI
|
|
11
|
Baxter AR, Newman E and Hajdu CH: Solitary
fibrous tumor of the pancreas. J Surg Case Rep. 2015:rjv1442015.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Yang W, Sun F, Liu H, Wang G, Shi P, Shao
Z and Guo F: Solitary fibrous tumors of the prostate: A case
report. Oncol Lett. 10:1617–1619. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Genc A, Toktas Z, Azman C, Bozkurt SU and
Kilic T: Solitary fibrous tumor of the orbit: A case report and
review of the literature. Turk Neurosurg. 25:984–987.
2015.PubMed/NCBI
|
|
14
|
Kim JH, Yang KH, Yoon PH and Kie JH:
Solitary fibrous tumor of central nervous system: A case report.
Brain Tumor Res Treat. 3:127–131. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Yu R and Rebello R: Solitary fibrous tumor
of the parotid gland: A case report. Iran J Otorhinolaryngol.
27:401–405. 2015.PubMed/NCBI
|
|
16
|
Abeygunasekera AM, Ginige AP and Liyanage
IS: A solitary fibrous tumor of the kidney. J Cancer Res Ther.
11:6622015. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Kawaguchi K, Taniguchi T, Usami N and
Yokoi K: Intrapulmonary solitary fibrous tumor. Gen Thorac
Cardiovasc Surg. 59:61–64. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Yang X, Jiang Q and Yu B: Solitary fibrous
tumor located in the sella turcica: A report of two cases and
review of the literature. Oncol Lett. 10:354–358. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Taguchi S: Primary cardiac solitary
fibrous tumors. Ann Thorac Cardiovasc Surg. 21:329–331. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Walker CT, Amene CS, Pannell JS,
Santiago-Dieppa DR, Rennert RC, Hansen LA and Khalessi AA:
Hemorrhagic intramedullary solitary fibrous tumor of the conus
medullaris: Case report. J Neurosurg Spine. 23:438–443. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Urabe M, Yamagata Y, Aikou S, Mori K,
Yamashita H, Nomura S, Shibahara J, Fukayama M and Seto Y: Solitary
fibrous tumor of the greater omentum, mimicking gastrointestinal
stromal tumor of the small intestine: A case report. Int Surg.
100:836–840. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Freiser ME, Castaño JE, Whittington EE,
Arnold DJ and Sidani CA: Solitary fibrous tumor of the
infratemporal fossa. J Radiol Case Rep. 8:1–8. 2014.PubMed/NCBI
|
|
23
|
Dozier J, Jameel Z, McCain DA, Hassoun P
and Bamboat ZM: Massive malignant solitary fibrous tumor arising
from the bladder serosa: A case report. J Med Case Rep. 9:462015.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Hyodo R, Komada T, Takada A, Kawai H, Ito
S, Nishida Y and Naganawa S: Solitary fibrous tumors in the
extremities: Imaging findings for six patients. Nagoya J Med Sci.
77:167–178. 2015.PubMed/NCBI
|
|
25
|
Kanazawa T, Kodama K, Nokubi M, Gotsu K,
Shinnabe A, Hasegawa M, Kusaka G and Iino Y: A case of solitary
fibrous tumor arising from the palatine tonsil. Ear Nose Throat J.
94:117–120. 2015.PubMed/NCBI
|
|
26
|
Ge W, Yu DC, Jiang CP and Ding YT: Giant
solitary fibrous tumor of the diaphragm: A case report and review
of literature. Int J Clin Exp Pathol. 7:9044–9049. 2014.PubMed/NCBI
|
|
27
|
Nishida K, Ubukata H, Konishi S, Shimazaki
J, Yano Y, Morishita Y and Tabuchi T: A giant solitary fibrous
tumor of the mesentery: A case report and literature review. World
J Surg Oncol. 13:172015. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Basaran R, Kaksi M, Onoz M, Balkuv E and
Sav A: Intradural solitary fibrous tumor of the lumbar spine: A
distinctive case report. Case Rep Neurol Med.
2015:7084722015.PubMed/NCBI
|
|
29
|
Tsubochi H, Endo T, Sogabe M, Endo S,
Morinaga S and Dobashi Y: Solitary fibrous tumor of the thymus with
variegated epithelial components. Int J Clin Exp Pathol.
7:7477–7484. 2014.PubMed/NCBI
|
|
30
|
de Oliveira DH, Albuquerque AF, de Araújo
Barreto MD, Nonaka CF, da Silva JS, Germano AR and Queiroz LM:
Large solitary fibrous tumor of the oral cavity-report of a case.
Pathol Res Pract. 210:1064–1067. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Hu S, Yi L, Yang L and Wang Y: Solitary
fibrous tumor of the spermatic cord: A case report and literature
review. Exp Ther Med. 9:55–58. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Vaziri M, Molanaei S and Tamannaei Z:
Solitary fibrous tumor of the intrathoracic goiter. Med J Islam
Repub Iran. 28:512014.PubMed/NCBI
|
|
33
|
Lee W, Jeon SM and Lee SH: Calcifying
fibrous tumor of the rectum: A case report. Indian J Pathol
Microbiol. 57:504–505. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Cho KJ, Ro JY, Choi J, Choi SH, Nam SY and
Kim SY: Mesenchymal neoplasms of the major salivary glands:
Clinicopathological features of 18 cases. Eur Arch
Otorhinolaryngol. 265 Suppl 1:S47–S56. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Gold JS, Antonescu CR, Hajdu C, Ferrone
CR, Hussain M, Lewis JJ, Brennan MF and Coit DG: Clinicopathologic
correlates of solitary fibrous tumors. Cancer. 94:1057–1068. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Alobid I, Bernal-Sprekelsen M, Benitez P,
Moragas M and Nadal A: Solitary fibrous tumor of the larynx.
Otolaryngol Head Neck Surg. 133:163–165. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Shim YS, Choi SJ, Kim HS and Lee JI:
Solitary fibrous tumor of the trachea: CT findings with a
pathological correlation. Korean J Radiol. 9:286–289. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Prévot S, Penna C, Imbert JC, Wendum D and
de Saint-Maur PP: Solitary fibrous tumor of the adrenal gland. Mod
Pathol. 9:1170–1174. 1996.PubMed/NCBI
|
|
39
|
Biedrzycki OJ, Singh N, Habeeb H, Wathen N
and Faruqi A: Solitary fibrous tumor of the female genital tract a
case report and review of the literature. Int J Gynecol Pathol.
26:259–264. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
O'Connel JX, Logan PM and Beauchamp CP:
Solitary fibrous tumors of the periosteum. Hum Pathol. 26:460–462.
1995. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Plönes T, Kayser G and Passlick B:
Solitary malignant fibrous tumor of the mediastinum. Asian
Cardiovasc Thorac Ann. 21:491–492. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Thompson CF, Bhuta SM and Abemayor E:
Solitary fibrous tumor of the hypopharynx: Case report and
literature review. Am J Otolaryngol. 34:545–547. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Cardinale L, Ardissone F, Cataldi A,
Familiari U, Solitro F and Fava C: Solitary fibrous tumor of the
lung: Three rare cases of intraparenchymal nodules. Acta Radiol.
50:379–382. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Ikeda T, Wada N, Nomura M, Tamiya S and
Ushijima M: A case of solitary fibrous malignant tumor with
multiple metastases. Nihon Kokyuki Gakkai Zasshi. 49:913–916.
2011.(In Japanese). PubMed/NCBI
|
|
45
|
Sironi M, Rho B and Spinelli M:
Adenofibromatous pattern in a solitary fibrous tumor of the lung.
Int J Surg Pathol. 13:792005. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Dong A, Zuo C, Wang Y and Cui Y: Enhanced
CT and FDG PET/CT in malignant solitary fibrous tumor of the lung.
Clin Nucl Med. 39:488–491. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
van de Rijn M, Lombard CM and Rouse RV:
Expression of CD34 by solitary fibrous tumors of the pleura,
mediastinum and lung. Am J Surg Pathol. 18:814–820. 1994.
View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Demırağ F, Cakir E and Alpar S: Expression
of CD44 and MMP-2: Possible association with histopathological
features of pleuro-pulmonary solitary fibrous tumors. Am J Surg.
18:814–820. 1994.
|
|
49
|
Barrettara B, Napoli G, Lacitignola A and
Sardelli P: Fibrous lung tumor: A peculiar case. J Thorac Dis.
5:E179–E180. 2013.PubMed/NCBI
|
|
50
|
Patsios D, Hwang DM and Chung TB:
Intraparenchymal solitary fibrous tumor of the lung: An uncommon
cause of a pulmonary nodule. J Thorac Imaging. 21:50–53. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Sakurai H, Tanaka W, Kaji M, Yamazaki K
and Suemasu K: Intrapulmonary localized fibrous tumor of the lung:
A very unusual presentation. Ann Thorac Surg. 86:1360–1362. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Sagawa M, Ueda Y, Matsubara F, Sakuma H,
Yoshimitsu Y, Aikawa H, Usuda K, Minato H and Sakuma T:
Intrapulmonary solitary fibrous tumor diagnosed by
immunohistochemical and genetic approaches: Report of a case. Surg
Today. 37:423–425. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Geramizadeh B, Banani A, Moradi A,
Hosseini SM and Foroutan H: Intrapulmonary solitary fibrous tumor
with bronchial involvement: A rare case report in a child. J
Pediatr Surg. 45:249–251. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Rao N, Colby TV, Falconieri G, Cohen H,
Moran CA and Suster S: Intrapulmonary solitary fibrous tumors:
Clinicopathologic and immunohistochemical study of 24 cases. Am J
Surg Pathol. 37:155–166. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
55
|
Caruso RA, LaSpada F, Gaeta M, Minutoli I
and Inferrera C: Report of an intrapulmonary solitary fibrous
tumor: Fine-needle aspiration cytologic findings,
clinicopathological and immunohistochemical features. Diagn
Cytopathol. 14:64–67. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Fridlington J, Weaver J, Kelly B and Kelly
E: Secondary hypertrophic osteoarthropathy associated with solitary
fibrous tumor of the lung. J Am Acad Dermatol. 57 Suppl
5:S106–S110. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
57
|
Kouki HS, Koletsis EN, Zolota V, Prokakis
C, Apostolakis E and Dougenis D: Solitary fibrous tumor of the
lung. Gen Thorac Cardiovasc Surg. 56:249–251. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
58
|
Baliga M, Flowers R, Heard K, Siddiqi A
and Akhtar I: Solitary fibrous tumor of the lung: A case report
with a study of the aspiration biopsy, histopathology,
immunohistochemistry and autopsy findings. Diagn Cytopathol.
35:239–244. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
59
|
Khalifa MA, Montgomery EA, Azumi N, Gomes
MN, Zeman RK, Min KW and Lack EE: Solitary fibrous tumors: A series
of lesions, some in unusual sites. South Med J. 90:793–799. 1997.
View Article : Google Scholar : PubMed/NCBI
|
|
60
|
Chang YL, Lee YC and Wu CT: Thoracic
solitary fibrous tumor: Clinical and pathological diversity. Lung
Cancer. 23:53–60. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
61
|
Musyoki FN, Nahal A and Powell TI:
Solitary fibrous tumor: An update on the spectrum of extrapleural
manifestations. Skeletal Radiol. 41:5–13. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
62
|
Klemperer P and Rabin CB: Primary
neoplasms of the pleura. A report of five cases. Arch Pathol.
11:385–412. 1931.
|
|
63
|
Yan J, Jones RL, Lewis DH and Eary JF:
Impact of (18)F-FDG PET/CT imaging in therapeutic decisions for
malignant solitary fibrous tumor of the pelvis. Clin Nucl Med.
38:453–455. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
64
|
Choi IH, Song DH, Han KM, Choi YS and Han
J: Incidence of pulmonary non-epithelial tumors: 18 years'
experience at a single institute. Pathol Res Pract. 210:210–216.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
65
|
Schirosi L, Lantuejoul S, Cavazza A, Murer
B, Brichon Yves P, Migaldi M, Sartori G, Sgambato A and Rossi G:
Pleuro-pulmonary solitary fibrous tumors: A clinicopathologic,
immunohistochemical and molecular study of 88 cases confirming the
prognostic value of de Perrot staging system and p53 expression and
evaluating the role of c-kit, BRAF, PDGFRs (alpha/beta), c-met and
EGFR. Am J Surg Pathol. 32:1627–1642. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
66
|
Gonullu G, Sullu Y, Basoglu A, Elmali M,
Karaoglanoglu M and Yucel I: Metastatic breast carcinoma to
solitary fibrous tumor in the lung. Indian J Cancer. 47:76–78.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
67
|
Strickland KC, Nucci MR, Esselen KM, Muto
MG, Chopra S, George S and Howitt BE: Solitary fibrous tumor of the
uterus presenting with lung metastases: A case report. Int J
Gynecol Pathol. 35:25–29. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
68
|
Míguez González J, Porres Varona D,
Soriano Andreu J and Fernández Montero MÁ: Intrapulmonary solitary
fibrous tumor associated with hemoptysis: A case report.
Radiologia. 54:182–186. 2012.(In Spanish). View Article : Google Scholar : PubMed/NCBI
|
|
69
|
Masuda R, Tanaka I, Inoue M, Furuhata Y
and Takemura T: Two cases of a solitary fibrous tumor with
different growth patterns. Nihon Kyobu Geka Gakkai Zasshi.
44:2177–2182. 1996.(In Japanese). PubMed/NCBI
|
|
70
|
Radulescu D, Pripon S, Ciuleanu TE and
Radulescu LI: Malignant primary pulmonary tumor with
hemangiopericytoma-like features: Conventional hemangiopericytoma
versus solitary fibrous tumor. Clin Lung Cancer. 8:504–508. 2007.
View Article : Google Scholar : PubMed/NCBI
|