Introduction
Ovarian cancer is one of the most common female low
genital malignant cancers. A total of ~238,700 women are annually
diagnosed with this disease all over the world and ~151,900
associated fatalities (1). In
addition, epithelial ovarian cancer (EOC) accounts for 90% of all
types of ovarian cancer. Most of EOC is diagnosed at an advanced
stage [the International Federation of Gynecology and Obstetrics
(FIGO) III or IV stages] because of the lack of specific symptoms
and the absence of effective early diagnostic methods, which leads
to a poor prognosis (2,3). Recently serum biomarkers such as CA125
and HE4 have been used to monitor the progress and prognosis of the
EOC, and also to detect the recurrence of disease after operation
or chemotherapy (4,5). However, these biomarkers are neither
particularly specific nor extremely sensitive for predicting cancer
metastasis, recurrence and prognosis. Therefore, further studies to
find new biomarkers and to provide targeted therapy are very
important.
The myosin 9 (MYH9) gene encodes the heavy chain of
non-muscle myosin of class II, isoform A (also called NM IIA). The
MYH9 gene is localized on chromosome 22q12.3, spanning >106 kbp
and composed of 41 exons (6).
Several studies suggested that MYH9 plays a different role in
various types of cancers. Many studies propose that NM IIA
expression or its functions in neoplastic cells promote the
progression of various types of cancers (7–14).
However, the studies that obtained the strongest evidence of a
driving role of MYH9 alterations in oncogenesis found that this
gene acts as a tumor suppressor (15–17). In
addition, it was demonstrated that silencing of MYH9 induced
metastatic squamous cell carcinoma (SCC) in the skin and head and
neck with median latencies of 3 to 7 months, and ablation of MYH9
also led to development of skin SCC. Moreover, investigation of
mouse and human keratinocytes demonstrated that NM IIA deficiency
induced defective activation of the p53 protein upon DNA damage, as
a result of impaired p53 stability and nuclear localization, and
the authors found that 24–31% of human skin and head and neck SCCs
are characterized by no or very weak NM IIA expression. In
addition, analysis of data from The Cancer Genome Atlas indicated
that low MYH9 mRNA expression is associated with poor survival in
patients with head and neck SCC, therefore also supporting a role
for MYH9 as a tumor suppressor in humans. Notably, in the tongue
SCC (18) and in human invasive
lobular breast carcinoma (19), MYH9
acts as a tumor suppressor.
However, to the best of our knowledge there have
been no research about the role of MYH9 in ovarian cancer.
Therefore, in the preset study the aim was to study the role of
MYH9 expression in ovarian cancer and its clinicopathological and
prognostic correlations.
Materials and methods
Tissue specimens and patient
samples
A total of 265 paraffin-embedded ovarian cancer
tissues (saved at Department of Pathology in the Memorial Hospital
of Sun Yat-sen University; the women were aged between 18 and 89
years old) and 41 paratumor ovarian tissues (saved at the
Department of Pathology in the Memorial Hospital of Sun Yat-sen
University; the women were aged between 51 and 72 years old) from
March 2009 to December 2017 which had been pathologically confirmed
at the Memorial Hospital of Sun Yat-sen University were included in
this study, and all of the paraffin-embedded tissues were cut into
4 µm-thick tissues and made to paraffin section. Survival was
calculated from the operation date until 14 April 2018 when any
remaining survivors were censored. This trial obtained approval
from the Memorial Hospital of Sun Yat-sen University Ethics
Committee. All controls and patients (or relatives of patients who
already died) provided written informed consent.
Immunohistochemistry
The MYH9 expression levels in the human EOC tissues
were detected by immunohistochemical analysis. Briefly, the samples
were fixed in 4% formaldehyde for 12 h subsequently 4 µm-thick
paraffin-embedded sections (saved at −20°C) were incubated at 65°C
for 2 h, deparaffinized with xylene, rehydrated and microwaved in
antigen retrieval buffer. Next, high tension was used for antigen
retrieval and the specimens were treated with 3% hydrogen peroxide
in methanol to quench endogenous peroxidase activity, followed by
incubation with 1% bovine serum albumin (OriGene Technologies,
Inc.) to block non-specific binding (room temperature for 15 min),
and incubation with anti-rabbit MYH9 polyclonal antibody (1:100;
cat. no. 11128-1-AP; Proteintech, Inc.) at 4°C overnight. After
washing, the tissue sections were treated with secondary antibody
(goat anti-mouse/rabbit IgG, cat no: SP-9000,; 50 ul for each
section; OriGene Technologies, Inc,) for 2 h at room temperature,
then incubated with streptavidin horseradish peroxidase complex
(OriGene Technologies, Inc.) for 15 min at room temperature,
immersed in 3-amino-9-ethyl carbazole. The sections were then
counterstained with 10% Mayer's hematoxylin (2 min at room
temperature), dehydrated and mounted in Crystal Mount. A total of
two researchers evaluated the degree of immunostaining of each
formalin-fixed, paraffin-embedded section with light microscope
(×200 or ×400; Olympus). The score was due to both the proportion
of positively stained tumor cells and the intensity of staining.
The percentage of cancer cells was scored as follows: Sections with
<10% positive cancer cells were scored as 0; 10–50% positive
cancer cells were scored as 1; 50–75% positive cancer cells were
scored as 2; and >75% positive cancer cells were scored as, 3.
Meanwhile, the tissues were sorted into four grades based on
staining intensity, as follows: 0 indicated no staining; 1
indicated weak staining (light yellow); 2 moderate staining (yellow
brown); and 3 strong staining (brown). The staining index (0–9) was
calculated as the product of the proportion of positive cells
multiplied by the staining intensity score. The best cutoff value
was defined as follows: A staining score of ≥6 was considered to
have high MYH9 expression and a staining score of ≤4 indicated low
MYH9 expression (20).
Statistical analysis
All of the statistical analyses were carried out
with the statistical software package SPSS 21.0 (IBM, Corps.). Data
are presented as mean ± standard error of the mean. The
χ2 test and Fisher's exact test were used to analyze the
relationship between MYH9 protein expression levels and
clinicopathological characteristics. Patient survival was
determined by a Kaplan-Meier analysis and the differences were
counted by the log-rank test. Cox's proportional hazards regression
model was applied to the multivariate analysis. P<0.05 was
considered to indicate a statistically significant difference.
Results
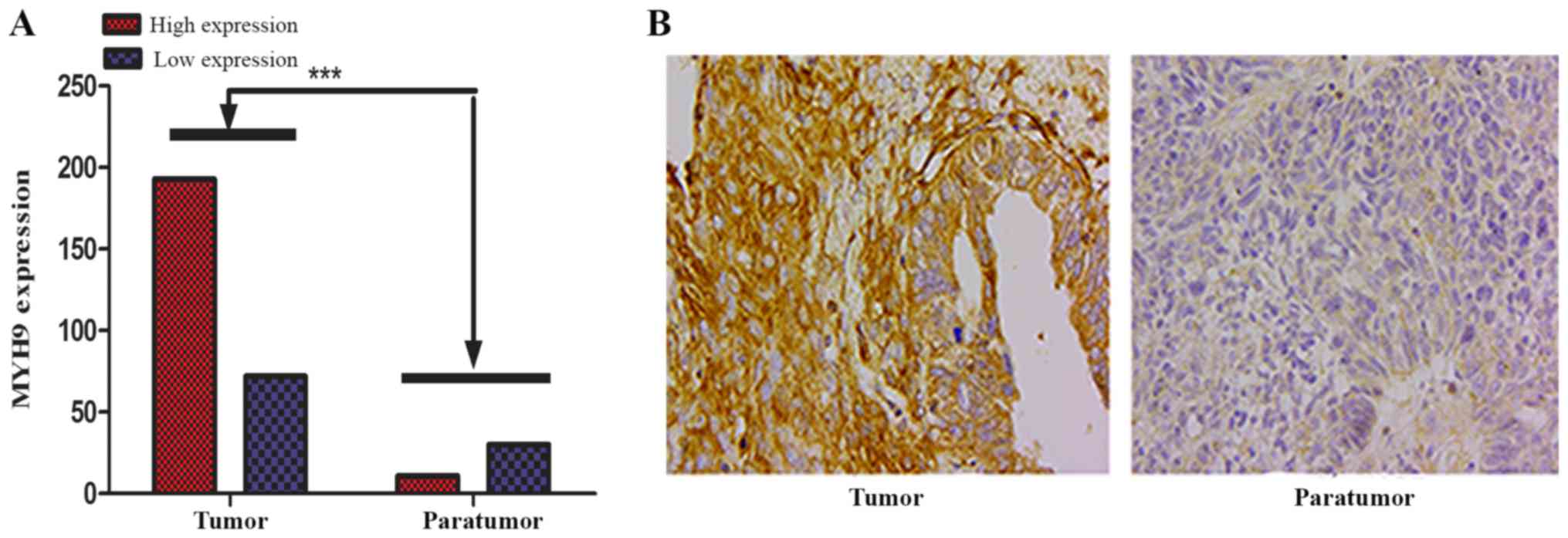
MYH9 protein expression is upregulated
in EOC
To determine whether MYH9 is a pro-tumor or
antitumor gene in ovarian cancer, immunohistochemical analysis was
performed in 265 cases of paraffin-embedded epithelial ovarian
cancer tissues and 41 cases of ovarian paratumor tissues. Of the
265 evaluable ovarian tumors stained, 72/265 (27.17%) had
weak/absent staining (also called low expression) and 193/265
(72.83%) had strong/moderate staining (also called high
expression). Moreover, of the 41 ovarian paratumor tissues stained,
30/41 (73.17%) had weak/absent staining (also called low
expression) and only 11/41 (26.83%) had strong/moderate staining
(also called high expression), and there was significantly
different staining between low and high MYH9 expression groups
(P<0.001; Fig. 1A). In addition,
it was demonstrated that MYH9 expression staining located in the
cytoplasm (Fig. 1B).
MYH9 overexpression is associated with
disease progression free and overall survival in ovarian cancer
patients
To determine whether the MYH9 expression was
associated with ovarian cancer patient's survival, in the present
study 265 cases of EOC were stained using immunohistochemistry with
a specific MYH9 antibody. Kaplan-Meier survival analysis
demonstrated that there was a significant difference in disease
progression free survival between high and low expression of MYH9
(P=0.004; Fig. 2). Moreover, there
was also a statistically significance on overall survival between
high and low MYH9 expression (Fig.
2). A survival analysis plot revealed that the cumulative
overall survival (OS) and disease progression free survival (PFS)
rates of ovarian cancer patients decreased with increasing MYH9
protein expression. In this study, patients with high expression of
MYH9 exhibited a median overall survival time of 24 months, while
patients with low expression of MYH9 exhibited a median overall
survival time of 41 months. Moreover, patients with MYH9 high
expression exhibited a median disease progression free survival
time of 12 months, while patients with MYH9 low expression
exhibited a median disease progression free survival time of 37
months.
Representative photomicrographs of the
EOC tissues immunohistochemically stained for MYH9
In 265 cases of ovarian cancer tissues stained with
the MYH9 specific antibody, 22 cases had no staining, 50 cases had
weak staining, 117 cases had moderate staining and 76 cases had
strong staining (Fig. 3). MYH9
expression is located at the cytoplasm and no expression at the
nucleus.
The association between MYH9
expression and clinicopathological variables
From Table I, it was
demonstrated that the percentages of patients with stages I, II,
III and IV tumors were 16.23, 10.19, 58.87, and 14.71%,
respectively, which demonstrated that most of epithelial ovarian
cancer was diagnosed at an advanced stage. In addition, most of
histological type is serous adenocarcinoma (69.87% in the present
study). In addition, The results of the statistical analysis using
χ2 or Fisher's Exact test demonstrated a significant
relationship between MYH9 expression and clinicopathological
characteristics of EOC, such as the following factors: FIGO stage,
lymph node metastasis, intraperitoneal metastasis, vital status (at
last follow-up), intraperitoneal recurrence, residual tumor size,
and ascites with tumor cells (P<0.05; Table I). Moreover, there were no
significance in the following factors: Age, histological type,
intestinal metastasis, distant recurrence, differentiation grade,
neoadjuvant chemotherapy, postoperative chemotherapy, platinum
resistance, hyperthermic intraperitoneal chemotherapy,
cytoreductive surgery, serum CA125, CA72-4, carcinoembryonic
antigen, α-fetoprotein, CA153 and human epididymis protein 4.
 | Table I.Association between MYH9 expression
and clinicopathological variables using the χ2 or
Fisher's exact test. |
Table I.
Association between MYH9 expression
and clinicopathological variables using the χ2 or
Fisher's exact test.
|
|
| MYH9 |
|
|
|---|
|
|
|
|
|
|
|---|
| Characteristic | Total, n (%) | No or low
expression | Moderate or strong
expression | χ2 test
P-value | Fisher's exact test
P-value |
|---|
| Age, years |
| ≤50 | 122 (46.04) | 39 | 83 | 0.1049 |
|
|
>50 | 143 (53.96) | 33 | 110 |
|
|
| Histological
type |
| Serous
adenocarcinoma | 160 (69.87) | 38 | 122 | 0.0684 |
|
| Mucoid
adenocarcinoma | 13
(5.68) | 5 | 8 |
|
|
|
Endometrial
adenocarcinoma | 38
(16.59) | 13 | 25 |
|
|
| Clear
cell carcinoma | 18
(7.86) | 9 | 9 |
|
|
| FIGO stage |
| I | 43
(16.23) | 17 | 26 | 0.0011 |
|
| II | 27
(10.19) | 14 | 13 |
|
|
| III | 156 (58.87) | 35 | 121 |
|
|
| IV | 39
(14.71) | 6 | 33 |
|
|
| Lymph node
metastasis |
| No | 61
(58.10) | 30 | 31 | 0.0059 |
|
| Yes | 44
(41.90) | 10 | 34 |
|
|
| Intraperitoneal
metastasis |
| No | 87
(32.95) | 39 | 48 | <0.0001 |
|
| Yes | 177 (67.05) | 33 | 144 |
|
|
| Intestinal
metastasis |
| No | 135 (51.14) | 39 | 96 | 0.5464 |
|
| Yes | 129 (48.86) | 33 | 96 |
|
|
| Vital status |
|
Alive | 111 (57.81) | 46 | 65 | <0.0001 |
|
| Dead | 81
(42.19) | 12 | 69 |
|
|
| Intraperitoneal
recurrence |
| No | 186 (71.81) | 60 | 126 | 0.0053 |
|
| Yes | 73
(28.19) | 11 | 62 |
|
|
| Distant
recurrence |
| No | 222 (85.71) | 64 | 158 | 0.2109 |
|
|
Yes | 37
(14.29) | 7 | 30 |
|
|
| Residual tumor size
(cm) |
| ≤1 | 241 (90.94) | 70 | 171 | 0.0296 | 0.0302 |
|
>1 | 24
(9.06) | 2 | 22 |
|
|
| Differentiation
grade |
|
G1/G2 | 96
(39.51) | 28 | 68 | 0.4184 |
|
| G3 | 147 (60.49) | 36 | 111 |
|
|
| Neoadjuvant
chemotherapy |
| No | 234 (88.30) | 67 | 167 | 0.1414 | 0.1967 |
|
Yes | 31
(11.70) | 5 | 26 |
|
|
| Postoperative
chemotherapy |
| No | 8
(3.05) | 1 | 7 |
| 0.4520 |
|
Yes | 254 (96.95) | 71 | 183 |
|
|
| Platinum
resistance |
| No | 255 (97.33) | 70 | 185 |
| >0.05 |
|
Yes | 7
(2.67) | 2 | 5 |
|
|
| Hyperthermic
intraperitoneal chemotherapy |
| No | 240 (90.91) | 65 | 175 | 0.8270 |
|
|
Yes | 24
(9.09) | 7 | 17 |
|
|
| Ascites with tumor
cells (+) |
| No | 56
(50.91) | 24 | 32 | 0.0058 |
|
|
Yes | 54
(49.09) | 10 | 44 |
|
|
| Cytoreductive
surgery |
| No | 9
(3.42) | 1 | 8 | 0.2655 | 0.4515 |
|
Yes | 254 (96.58) | 71 | 183 |
|
|
| CA125 (U/ml) |
|
≤35 | 32
(12.65) | 11 | 21 | 0.3060 |
|
|
>35 | 221 (87.35) | 57 | 164 |
|
|
| CA72-4 (U/ml) |
| ≤7 | 99
(45.83) | 30 | 69 | 0.4459 |
|
|
>7 | 117 (54.17) | 30 | 87 |
|
|
| CA153 (U/ml) |
|
≤25 | 31
(32.29) | 6 | 25 | 0.5664 |
|
|
>25 | 65
(67.71) | 16 | 49 |
|
|
| AFP (U/ml) |
|
≤25 | 209 (99.05) | 59 | 150 |
| >0.05 |
|
>25 | 2
(0.95) | 0 | 2 |
|
|
| CEA (U/ml) |
|
≤5.0 | 189 (88.32) | 54 | 135 | 0.9526 |
|
|
>5.0 | 25
(11.68) | 7 | 18 |
|
|
| HE4 (pmol/l) |
|
≤140 | 45
(34.35) | 16 | 29 | 0.6301 |
|
|
>140 | 86
(65.65) | 27 | 59 |
|
|
MYH9 overexpression is significantly
associated with a poor prognosis
Furthermore, the prognostic value of MYH9 expression
in EOC patients were also analyzed. In a univariate Cox analysis,
MYH9 expression, intraperitoneal metastasis, intestinal metastasis,
postoperative chemotherapy and hyperthermic intraperitoneal
chemotherapy were significant prognostic factors (P<0.05;
Table II). Moreover, using a
multivariate Cox regression analysis found that MYH9
expression, intestinal metastasis, postoperative chemotherapy and
hyperthermic intraperitoneal chemotherapy were indeed independent
prognostic factors of ovarian cancer (Table II), but intraperitoneal metastasis
was no longer significant (P=0.570). Taken together, these results
suggest that MYH9 expression was an independent prognostic factor
and MYH9 overexpression may be corelated with the prognosis of
epithelial ovarian cancer, which suggested that MYH9 may be a
useful independent prognostic marker in EOC.
| Table II.Cox regression univariate and
multivariate analyses of prognostic factors in epithelial ovarian
cancer. |
Table II.
Cox regression univariate and
multivariate analyses of prognostic factors in epithelial ovarian
cancer.
|
| Univariate
analysis | Multivariate
analysis |
|---|
|
|
|
|
|---|
| Variable | Number of
patients | P-value | Regression
coefficient (SE) | P-value | 95% confidence
interval |
|---|
| MYH9 |
| Low
expression | 72 | 0.007 | 0.339 | 0.009 | 1.250–4.802 |
| High
expression | 193 |
|
|
|
|
| Intraperitoneal
metastasis |
| No | 87 | 0.026 | 0.320 | 0.570 | – |
|
Yes | 177 |
|
|
|
|
| Intestinal
metastasis |
| No | 135 | 0.040 | 0.250 | 0.011 | 1.176–3.422 |
|
Yes | 129 |
|
|
|
|
| Postoperative
chemotherapy |
| No | 8 | 0.004 | 0.639 | <0.001 | 0.024–0.347 |
|
Yes | 254 |
|
|
|
|
| Hyperthermic
intraperitoneal chemotherapy |
| No | 240 | 0.007 | 0.485 | 0.026 | 1.138–7.935 |
|
Yes | 24 |
|
|
|
|
Discussions
The MYH9 gene encodes the heavy chain of non-muscle
myosin of class II, isoform A (also called NM IIA). MYH9 plays a
different role in human cancers (4–15). MYH9
plays an oncogenic role in a number of types of cancers (5–12), such
as gastric cancer, colorectal cancer, esophageal squamous cancer,
non-small cell lung cancer and breast cancer. However, in contrast,
it plays a tumor suppressor in a number of cancers (13–15),
such as human skin and head and neck SCCs, tongue SCC and human
invasive lobular breast carcinoma. However, there have been no
studies about the role of MYH9 in ovarian cancer. In this study the
authors for the first time to the best of our knowledge
demonstrated that MYH9 protein expression was elevated in
EOC tissues and out of 265 evaluable ovarian tumors stained, 72/265
(27.17%) had weak/absent staining and 193/265 (72.83%) had
strong/moderate staining (also called high expression). However,
out of 41 ovarian paratumor tissues stained, 30/41 (73.17%) had
weak/absent staining (also called low expression) and only 11/41
(26.83%) had strong/moderate staining (also called high
expression), which suggested that MYH9 may play an oncogenic role
in EOC. As is known, EOC is an adenocarcinoma pathologically and in
previous studies MYH9 was demonstrated to play a tumor suppressor
role in a number of squamous carcinomas (15–17). The
present study demonstrated the same discrepancy as with the
previous studies (7–14). In addition, survival analysis
revealed that the cumulative OS and PFS rates of EOC patients
decreased with increasing MYH9 protein expression, and high
expression of MYH9 exhibited a poorer median OS and PFS, which
demonstrated that MYH9 overexpression predicts a poor prognosis of
EOC.
Moreover, overexpression of MYH9 in EOC patients was
found to be associated with the following factors, such as FIGO
stage, lymph node metastasis, intraperitoneal metastasis, vital
status (at last follow-up), intraperitoneal recurrence, residual
tumor size and ascites with tumor cells. In the present study, it
was demonstrated that patients with MYH9 overexpression were
more frequently in stage III/IV compared with stage I/II, which
demonstrated that MYH9 overexpression were more likely to be
associated with advanced disease, therefore it was concluded that
MYH9 expression increased with the occurrence and progress of
ovarian cancer. Moreover, MYH9 overexpression was associated with
lymph node metastasis and intraperitoneal metastasis, which
demonstrated that high expression of MYH9 was associated with the
metastasis of epithelial ovarian cancer. In addition,
intraperitoneal recurrence occurred more frequently in the MYH9
high expression group, which showed that MYH9 overexpression was
associated with the recurrence of EOC. As far as the authors know,
EOC metastasis and recurrence are the major mortality factors, and
patients with metastasis and recurrence usually have a shorter life
span. Therefore, early diagnosis of metastasis and recurrence is
important for prolonging the survival of ovarian cancer patients,
however there are few tumor markers for predicting metastasis and
recurrence of ovarian cancer in the clinic. According to the
results of the present study, MYH9 overexpression was associated
with lymph node metastasis, intraperitoneal metastasis and
recurrence, and is meaningful as a biomarker or predictor to
diagnose lymph node metastasis, intraperitoneal metastasis and
recurrence. All of these results suggested that MYH9 overexpression
is associated with a poor prognosis of EOC and it could be
recommended as a candidate molecular biomarker of EOC. Moreover, it
was concluded that MYH9 may directly or indirectly participate in
the migration and invasion of ovarian cancer. However, more in
vivo and in vitro experiments are required to identify
its role in EOC.
Furthermore, using univariate Cox analysis it was
found that MYH9 expression, intraperitoneal metastasis, intestinal
metastasis, postoperative chemotherapy and hyperthermic
intraperitoneal chemotherapy were prognostic factors. In addition,
in a multivariate Cox regression analysis demonstrated that
MYH9 expression, intestinal metastasis, postoperative
chemotherapy and hyperthermic intraperitoneal chemotherapy were
independent prognostic factors of ovarian cancer, but
intraperitoneal metastasis was not significantly associated. All
these results suggest that MYH9 expression is an independent
prognostic factor and MYH9 overexpression may be corelated with the
prognosis of EOC, which suggested that MYH9 may be a useful
independent prognostic marker in EOC. In addition, intraperitoneal
metastasis and intestinal metastasis were associated with poor
prognosis of EOC, so more efficacious treatment methods should be
given to these patients. Moreover, the present study suggested that
hyperthermic intraperitoneal chemotherapy should be performed in
cytoreductive surgery, because it influences the prognosis of
EOC.
In conclusion, MYH9 overexpression was associated
with FIGO stage, lymph node metastasis, intraperitoneal metastasis,
vital status, intraperitoneal recurrence, residual tumor size and
ascites with tumor cells. Additionally, it was an independent
prognostic factor and its overexpression may be associated with the
poor prognosis of ovarian cancer. Furthermore, MYH9 can be
recommended as a useful independent prognostic marker in EOC. In
future, more in vivo and in vitro studies are
required to demonstrate its role and molecular mechanism in
development and progression of ovarian cancer.
Acknowledgements
The authors would like to thank Professor Zhongqiu
Lin for providing ovarian cancer and paratumor paraffin-embedded
tissues.
Funding
The present study was supported by the Nature
Science Fund of Guangdong Province (grant no. 2016A030313536) and
the Guangdong Provincial Medical Research Fund (grant no.
A2019096).
Availability of data and materials
All data generated or analyzed during this study are
included in this published article.
Authors' contributions
ZZ conceived and designed the experiments. LL and
JJY performed the experiments. XD, JHY and BZ analyzed the data. ZL
was involved in preparing paraffin-embedded ovarian cancer tissue
samples. LL wrote the paper. All authors have read and approved the
final manuscript.
Ethics approval and consent to
participate
The Ethics Committee of the Memorial Hospital of Sun
Yat-sen University authorized the experimental and research
protocols of this study. All procedures performed in studies were
in accordance with the ethical standards of the institutional
and/or national research committee and with the 1964 Helsinki
declaration and its later amendments or comparable ethical
standards. All controls and patients (or relatives of patients who
already died) provided written informed consent.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Jemal A, Bray F, Center MM, Ferlay J, Ward
E and Forman D: Global cancer statistics. CA Cancer J Clin.
61:69–90. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Weberpals JI, Koti M and Squire JA:
Targeting genetic and epigenetic alterations in the treatment of
serous ovarian cancer. Cancer Genet. 204:525–535. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Jayson GC, Kohn EC, Kitchener HC and
Ledermann JA: Ovarian cancer. Lancet. 384:1376–1388. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Ahmed AA and Abdou AM: Diagnostic accuracy
of CA125 and HE4 in ovarian carcinoma patients and the effect of
confounders on their serum levels. Curr Probl Cancer.
S0147-0272(18)30164-8. 2019. View Article : Google Scholar
|
|
5
|
Dochez V, Caillon H, Vaucel E, Dimet J,
Winer N and Ducarme G: Biomarkers and algorithms for diagnosis of
ovarian cancer: CA125, HE4, RMI and ROMA, a review. J Ovarian Res.
12:282019. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Pecci A, Ma X, Savoia A and Adelstein RS:
MYH9: Structure, functions and role of non-muscle myosin IIA in
human disease. Gene. 664:152–167. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Liang S, He L, Zhao X, Miao Y, Gu Y, Guo
C, Xue Z, Dou W, Hu F, Wu K, et al: MicroRNA let-7f inhibits tumor
invasion and metastasis by targeting MYH9 in human gastric cancer.
PLoS One. 6:e184092011. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Park SY, Kim H, Yoon S, Bae JA, Choi SY,
Jung YD and Kim KK: KITENIN-targeting microRNA-124 suppresses
colorectal cancer cell motility and tumorigenesis. Mol Ther.
22:1653–1664. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Xia ZK, Yuan YC, Yin N, Yin BL, Tan ZP and
Hu YR: Nonmuscle myosin IIA is associated with poor prognosis of
esophageal squamous cancer. Dis Esophagus. 25:427–436. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Hosono Y, Usukura J, Yamaguchi T,
Yanagisawa K, Suzuki M and Takahashi T: MYBPH inhibits NM IIA
assembly via direct interaction with NMHC IIA and reduces cell
motility. Biochem Biophys Res Commun. 428:173–178. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Katono K, Sato Y, Jiang SX, Kobayashi M,
Nagashio R, Ryuge S, Fukuda E, Goshima N, Satoh Y, Saegusa M and
Masuda N: Prognostic significance of MYH9 expression in resected
non-small cell lung cancer. PLoS One. 10:e01214602015. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Derycke L, Stove C, Vercoutter-Edouart AS,
De Wever O, Dollé L, Colpaert N, Depypere H, Michalski JC and
Bracke M: The role of non-muscle myosin IIA in aggregation and
invasion of human MCF-7 breast cancer cells. Int J Dev Biol.
55:835–840. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Liao Q, Li R, Zhou R, Pan Z, Xu L, Ding Y
and Zhao L: LIM kinase 1 interacts with myosin-9 and
alpha-actinin-4 and promotescolorectal cancer progression. Br J
Cancer. 117:563–571. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Ye G, Huang K, Yu J, Zhao L, Zhu X, Yang
Q, Li W, Jiang Y, Zhuang B, Liu H, et al: MicroRNA-647 targets
SRF-MYH9 axis to suppress invasion and metastasis of gastric
cancer. Theranostics. 7:3338–3353. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Schramek D, Sendoel A, Segal JP, Beronja
S, Heller E, Oristian D, Reva B and Fuchs E: Direct in vivo RNAi
screen unveils myosin IIa as a tumor suppressor of squamous cell
carcinomas. Science. 343:309–313. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Coaxum SD, Tiedeken J, Garrett-Mayer E,
Myers J, Rosenzweig SA and Neskey DM: The tumor suppressor
capability of p53 is dependent on non-muscle myosin IIA function in
head and neck cancer. Oncotarget. 8:22991–23007. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Wei XH, Lin SS, Liu Y, Zhao RP, Khan GJ,
Du HZ, Mao TT, Yu BY, Li RM, Yuan ST and Sun L: DT-13 attenuates
human lung cancer metastasis via regulating NMIIA activity under
hypoxia condition. Oncol Rep. 36:991–999. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Conti MA, Saleh AD, Brinster LR, Cheng H,
Chen Z, Cornelius S, Liu C, Ma X, Van Waes C and Adelstein RS:
Conditional deletion of nonmuscle myosin II-A in mouse tongue
epithelium results in squamous cell carcinoma. Sci Rep.
5:140682015. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Kas SM, de Ruiter JR, Schipper K,
Annunziato S, Schut E, Klarenbeek S, Drenth AP, van der Burg E,
Klijn C, Ten Hoeve JJ, et al: Insertional mutagenesis identifies
drivers of a novel oncogenic pathway in invasive lobular breast
carcinoma. Nat Genet. 49:1219–1230. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Liu L, Zeng Z, Yi J, Zuo L, Lv J, Yuan J,
Lin Z, Luo R and Feng X: Expression and clinical significance of
transcription factor 4 (TCF4) in epithelial ovarian cancer. Cancer
Biomark. 24:213–221. 2019. View Article : Google Scholar : PubMed/NCBI
|