Introduction
Since the 1970s, the incidence of renal cell
carcinoma (RCC) has increased by an annual mean rate of 3–4%, which
in turn was associated with a more prevalent use of various
radiological imaging methods for the evaluation of diverse
abdominal problems (1,2). It has been reported that 20–30% of
patients with RCC exhibit metastatic RCC (3). In addition, 20–30% of patients who
undergo nephrectomy for clinically localized disease progressively
metastasize during follow-ups (4).
Therefore, when RCC is diagnosed, it is necessary to evaluate the
presence or absence of metastasis. The foremost metastatic site of
RCC is the lung, which is involved in 45–75% of metastatic cases
(5). Therefore, when determining the
presence or absence of metastasis from RCC, the first priority
should be to evaluate pulmonary metastasis.
In a number of cases, at the time of RCC diagnosis,
pulmonary nodules were detected through chest radiological imaging
(6–8).
The significance of these pulmonary nodules remains unclear.
Additionally, these pulmonary nodules are frequently defined as
indeterminate by radiologists and are generally too small to
perform percutaneous biopsy (9).
Therefore, physicians and patients have not demonstrated a notable
interest in these pulmonary nodules. However, pulmonary nodules may
serve an important role in lung metastasis. Non-calcified pulmonary
nodules may represent metastatic disease in 19% of patients
diagnosed with cancer (10).
Evidently, this association, to the best of our knowledge, has not
been noticed nor studied in detail. Despite the association between
pulmonary nodules and lung cancer, pulmonary nodules located
through preoperative chest radiological imaging are frequently
overlooked, and their presence generally does not influence
postoperative follow-up protocols. Current American Urological
Association guidelines for the follow-up imaging (radiography and
chest) of patients who undergo surgery for clinically localized
renal masses are based on disease risk as defined by the pathologic
tumor stage (11), emphasizing its
overall importance. The purpose of the present study was to outline
and elaborate prognostic indicators of pulmonary metastasis and to
clarify the association between pulmonary nodules and pulmonary
metastasis in patients with RCC.
Patients and methods
Patient population
This was a retrospective study, and the study
protocols were approved by the Medical Ethics Committee of the
Institutional Review Board of Pusan National University Hospital
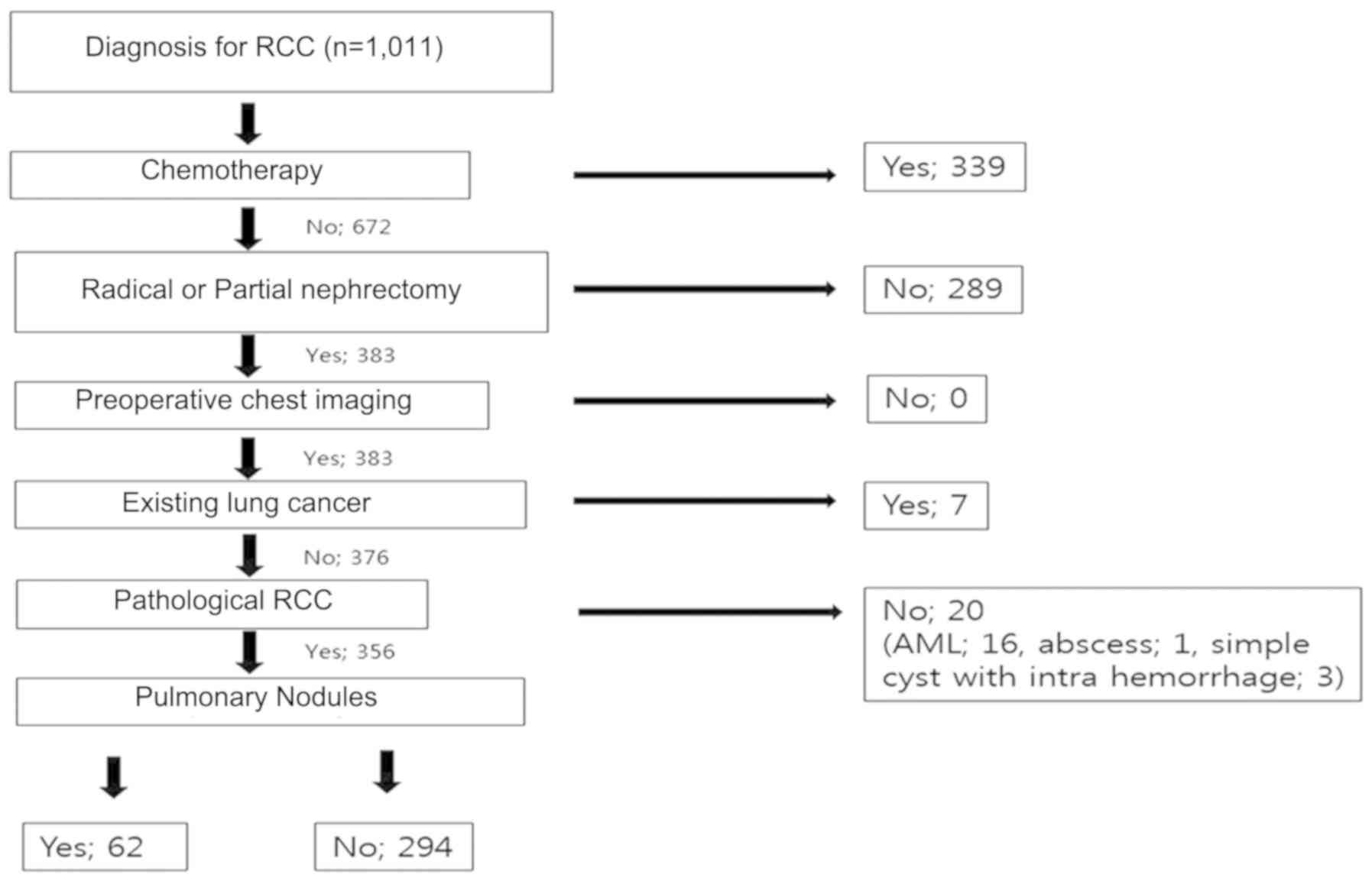
(Busan, Korea). Out of the 1,011 patients diagnosed with RCC, the
present study included 383 patients, who had undergone radical or
partial nephrectomy for RCC at the Pusan National University
Hospital between 2011 and 2016. The probability of lung metastasis
for each lesion was evaluated with a two-point confidence scale,
with Fig. 1 representing a metastatic
lesion, and Fig. 2 representing a
benign or indeterminate lesion. On the chest computed tomographic
(CT) image, the metastatic nodule was characterized as a lesion
with a well-circumscribed border, round shape, soft tissue
attenuation and/or multiplicity. Therefore, during imaging
analysis, the binary values were assigned for the characterization
of the pulmonary nodule. Nodules exhibiting features of metastatic
nodule were assigned to 1, whereas nodules exhibiting benign or
indeterminate features were assigned to 2 (5,10,12). The last follow-up was conducted on
March 31st 2018. Exclusion criteria for the patient sample
collection were as follows: Patients who underwent chemotherapy;
patients who did not undergo renal resection or preoperative chest
CT; and patients who were already diagnosed with pulmonary
metastasis prior to surgery. Following surgery, patients who were
diagnosed by pathology as benign tumor in the kidney were excluded
from the present study (Fig. 3).
The data from 356 patients, 243 male and 113 female
patients (59.3±12.3 and 58.1±12.3, respectively) were used and
patients were divided into the following 2 groups: Absent (n=323)
and present (n=33), according to the status of pulmonary
metastasis. Patient characteristics were examined, including age,
sex, body mass index (BMI), presence of pulmonary nodules, smoking
status, diabetes mellitus (DM), hypotension (HTN), renal tumor
size, renal tumor site, renal tumor location, renal vein thrombus
status, serum creatinine levels, albumin, lactate dehydrogenase
(LDH), hemoglobin, calcium, potassium, symptomatic flank pain,
pathologic T stage (pTstage), pathologic N stage, histologic
subtype (clear cell vs. non-clear cell), lymphovascular invasion,
presence of sarcomatoid cells and renal fat invasion status, using
the patients' medical records. The patients underwent chest CT
every 3–6 months following renal surgery. If pulmonary nodules were
detected through preoperative chest CT, the size, number, site, and
location of the nodules was examined. The size of the pulmonary
nodules was defined as the longest diameter on an axial image.
Following surgery, pathology reports were used to determine the
tumor-node-metastasis classification (11) of malignant tumors and the histologic
subtype. Written informed consent was obtained from all patients
prior to enrollment in the study, in addition to explaining its
purpose and methods.
Statistical analysis
An Continuous variables were described by mean ±
standard deviation and median (range), and qualitative variables by
size and percentage. Independent Student's t-test was used for
numerical patient data, including age, BMI, renal tumor size, serum
creatinine, albumin, LDH, hemoglobin, calcium, potassium, and
pulmonary nodule size. Fisher's exact test or χ2 test
was used for categorical data, including sex, presence of pulmonary
nodule, smoking status, DM, HTN, renal tumor site and location,
renal vein thrombus, symptomatic flank pain, the number, site and
location of pulmonary nodules, pathological tumor and lymph node
stages, histologic subtype, lymphovascular invasion, presence of
sarcomatoid cells and renal fat invasion status. Univariate and
multivariate logistic regression analyses and log-rank test were
used to assess the association between each of the factors and
progression to pulmonary metastasis. P<0.05 was considered to
indicate a statistically significant difference. All data were
analyzed using SPSS 20.0 software (IBM Corp., Armonk, NY, USA).
Results
Clinicopathological
characteristics
A total of 1,011 patients with RCC diagnosed by
abdomen CT were included in the present study. Among these, 383
patients underwent radical nephrectomy, and 356 patients were
included in the criteria. The median follow-up duration was 54.4
months (interquartile range, 38.8–71.8). At the time of the last
follow-up, pulmonary nodules were absent from 294 patients and
present in 62 patients. Table I
includes the patient characteristics of the two groups (with and
without pulmonary metastasis). Patients with pulmonary metastasis
indicated statistically significant results for the following: Age
(P=0.011), larger renal tumor size (P=0.005), renal vein thrombus
(P<0.001), median albumin (P=0.002), pTstage (P<0.001),
pNstage (P<0.001), renal fat invasion (P<0.001), and the
status of pulmonary nodule (P<0.001). In addition, pulmonary
metastasis was observed in 24% of patients with pulmonary nodules.
There were no statistically significant differences between the two
groups in other factors regarding pulmonary nodule size.
 | Table I.Clinicopathological characteristics of
356 patients with renal cell carcinoma treated with
nephrectomy. |
Table I.
Clinicopathological characteristics of
356 patients with renal cell carcinoma treated with
nephrectomy.
|
|
| Pulmonary
metastasis |
|
|---|
|
|
|
|
|
|---|
| Variables | Total | Absent | Present | P-value |
|---|
| Number of patients,
(%) | 356 | 323 (90.7) | 33 (9.3) |
|
| Median age ± SD
(years) | 58.9±12.3 | 58.4±12.5 | 63.1±9.2 | 0.011 |
| Sex n, (%) |
|
|
| 0.992 |
| Male | 243 (68.3) | 221 (68.4) | 22 (66.7) |
|
|
Female | 113 (31.7) | 102 (31.6) | 11 (33.3) |
|
| Median BMI ± SD
(kg/m2) | 24.1±3.4 | 24.1±3.4 | 24.2±3.8 | 0.941 |
| Pulmonary nodule, n
(%) |
|
|
| <0.001 |
|
Absent | 294 (82.6) | 276 (85.4) | 18 (54.5) |
|
|
Present | 62 (17.4) | 47 (14.6) | 15 (45.5) |
|
| Smoker, n (%) |
|
|
| 0.925 |
|
Absent | 256 (71.9) | 233 (72.1) | 23 (69.7) |
|
|
Present | 100 (28.1) | 90 (27.9) | 10 (30.3) |
|
| DM, n (%) |
|
|
| 1.000 |
|
Absent | 311 (87.4) | 282 (87.3) | 29 (87.9) |
|
|
Present | 45 (12.6) | 41 (12.7) | 4 (12.1) |
|
| HTN, n (%) |
|
|
| 1.000 |
|
Absent | 221 (62.1) | 201 (62.2) | 20 (60.6) |
|
|
Present | 135 (37.9) | 122 (37.8) | 13 (39.4) |
|
| Median renal tumor
size ± SD (mm) | 38.9±24.2 | 37.3±23.0 | 53.6±30.7 | 0.005 |
| Renal tumor site, n
(%) |
|
|
| 0.948 |
|
Right | 160 (46.0) | 145 (46.5) | 15 (47.4) |
|
|
Left | 188 (54.0) | 170 (53.5) | 18 (52.6) |
|
| Renal tumor
location, n (%) |
|
|
| 0.249 |
|
Upper | 109 (32.6) | 94 (31.2) | 15 (45.5) |
|
|
Middle | 132 (39.5) | 121 (40.2.) | 11 (33.3) |
|
|
Lower | 93 (27.8) | 86 (28.6) | 7 (21.2) |
|
| Renal vein
thrombus, n (%) |
|
|
| <0.001 |
|
Absent | 333 (96.8) | 305 (98.1) | 28 (84.8) |
|
|
Present | 11 (3.2) | 6 (1.9) | 5 (15.2) |
|
| Median creatinine ±
SD (mg/dl) | 1.1±1.0 | 1.1±1.1 | 1.0±0.3 | 0.228 |
| Median albumin ± SD
(g/dl) | 3.7±0.6 | 3.7±0.6 | 3.5±0.4 | 0.002 |
| Median LDH ± SD
(IU/l) | 225.9±87.5 | 226.4±88.3 | 220.9±84.0 | 0.837 |
| Median hemoglobin ±
SD (g/dl) | 12.4±1.6 | 12.4±1.6 | 11.9±1.8 | 0.074 |
| Median calcium ± SD
(mg/dl) | 8.4±0.7 | 8.4±0.7 | 8.5±0.7 | 0.389 |
| Median K ± SD
(mmol/l) | 4.1±0.5 | 4.1±0.5 | 4.0±0.5 | 0.822 |
| Symptomatic flank
pain, n (%) |
|
|
| 0.246 |
|
Absent | 337 (96.0) | 308 (96.6) | 29 (90.6) |
|
|
Present | 14 (4.0) | 11 (3.4) | 3 (9.4) |
|
| Median pulmonary
nodule size ± SD (mm) | 9.0±8.5 | 8.4±8.9 | 10.7±6.9 | 0.359 |
| Pulmonary nodule
number, n (%) |
|
|
| 0.130 |
| 1 | 33 (53.2) | 25 (53.2) | 8 (53.3) |
|
| 2 | 14 (22.6) | 13 (27.7) | 1 (6.7) |
|
| 3 | 1 (1.6) | 1 (2.1) | 0 (0.0) |
|
| 4 | 0 (0.0) | 0 (0.0) | 0 (0.0) |
|
| 5 | 1 (1.6) | 0 (0.0) | 1 (6.7) |
|
|
>5 | 13 (21.0) | 8 (17.0) | 5 (33.3) |
|
| Pulmonary nodule
site, n (%) |
|
|
| 0.958 |
|
Right | 21 (33.9) | 18 (36.0) | 3 (25.0) |
|
|
Left | 18 (29.0) | 15 (30.0) | 3 (25.0) |
|
|
Bilateral | 23 (37.1) | 17 (34.0) | 6 (50.0) |
|
| Pulmonary nodule
location, n (%) |
|
|
| 0.394 |
|
Lower | 11 (17.7) | 10 (21.3) | 1 (6.7) |
|
|
Middle | 6 (9.7) | 5 (10.6) | 1 (6.7) |
|
|
Upper | 23 (37.1) | 15 (31.9) | 8 (53.3) |
|
|
Multiple | 22 (35.5) | 17 (36.2) | 5 (33.3) |
|
| 1pT
stage, n (%) |
|
|
| <0.001 |
|
pT1-T2 | 239 (82.7) | 226 (87.3) | 13 (43.3) |
|
|
pT3-T4 | 50 (17.3) | 33 (12.7) | 17 (56.7) |
|
| 2pN
stage, n (%) |
|
|
| <0.001 |
|
pN0 | 214 (82.9) | 200 (86.2) | 14 (53.8) |
|
| pN1
(27) | 44 (17.1) | 32 (13.8) | 12 (46.2) |
|
| Histologic subtype,
n (%) |
|
|
| 0.237 |
| Clear
cell | 241 (83.7) | 214 (82.6) | 27 (93.1) |
|
|
Non-clear cell | 47 (16.3) | 45 (17.4) | 2 (6.9) |
|
| Lymphovascular
invasion, n (%) |
|
|
| 0.107 |
|
Absent | 277 (92.6) | 251 (93.7) | 26 (83.9) |
|
|
Present | 22 (7.4) | 17 (6.3) | 5 (16.1) |
|
| Sarcomatoid
differentiation, n (%) |
|
|
| 0.960 |
|
Absent | 273 (98.2) | 248 (98.4) | 25 (96.2) |
|
|
Present | 5 (1.8) | 4 (1.6) | 1 (3.8) |
|
| Renal fat invasion,
n (%) |
|
|
| <0.001 |
|
Absent | 241 (90.6) | 223 (92.9) | 18 (69.2) |
|
|
Present | 25 (9.4) | 17 (7.1) | 8 (30.8) |
|
The factors associated with pulmonary
metastasis in patients with RCC
The results of univariate and multivariate logistic
regression analyses on progression to pulmonary metastasis in the
groups of patients with RCC are displayed in Table II. In univariate logistic regression
analysis, progression to pulmonary metastasis was significantly
associated with age [hazard ratio (HR)=1.03; 95% confidence
interval (CI), 1.00–1.07; P=0.0410], pulmonary nodules (HR=4.89;
95% CI, 2.29–10.39; P<0.001), renal tumor size (HR=1.02; 95% CI,
1.01–1.03; P=0.0007), renal vein thrombus (HR=9.08; 95% CI,
2.48–32.03; P=0.0005), albumin (HR=0.41; 95% CI, 0.21–0.81;
P=0.0094), pTstage (HR=8.96; 95% CI, 4.01–20.49; P<0.001), and
renal fat invasion (HR=5.83; 95% CI, 2.14–15.13; P=0.0004). In
multivariate logistic regression analysis, pulmonary nodule
(HR=3.15; 95% CI, 1.12–8.68; P=0.0262), albumin (HR=0.42; 95% CI,
0.17–1.03; P=0.0490) and pTstage (HR=3.63; 95% CI, 0.98–12.86;
P=0.0475) were significantly associated with pulmonary metastasis.
According to the Kaplan-Meier curves, there was a strong difference
(P<0.001) in progression to pulmonary metastasis in patients
with pulmonary nodules, compared with patients without pulmonary
nodules (Fig. 4).
| Table II.Prognostic indicators for progression
to pulmonary metastasis in patients with renal cell carcinoma. |
Table II.
Prognostic indicators for progression
to pulmonary metastasis in patients with renal cell carcinoma.
|
| Univariate
analysis | Multivariate
analysis |
|---|
|
|
|
|
|---|
| Factors | P-value | HR | 95% CI | P-value | HR | 95% CI |
|---|
| Age | 0.0410 | 1.03 | 1.00–1.07 | 0.0735 | 1.04 | 1.00–1.10 |
| Pulmonary
nodule | <0.001 | 4.89 | 2.29–10.39 | 0.0262 | 3.15 | 1.12–8.68 |
| Renal tumor
size | 0.0007 | 1.02 | 1.01–1.03 | 0.2702 | 1.01 | 0.99–1.03 |
| Renal vein
thrombus | 0.0005 | 9.08 | 2.48–32.03 | 0.9032 | 1.11 | 0.19–6.30 |
| Albumin | 0.0094 | 0.41 | 0.21–0.81 | 0.0490 | 0.42 | 0.17–1.03 |
| 1pTstage
(25) | <0.001 | 8.96 | 4.01–20.49 | 0.0475 | 3.63 | 0.98–12.86 |
| Renal fat
invasion | 0.0004 | 5.83 | 2.14–15.13 | 0.6316 | 1.41 | 0.33–5.87 |
The factors associated with pulmonary
metastasis in patients with RCC pulmonary nodule
In subgroup analysis, the risk factors associated
with pulmonary metastasis were examined in patients with pulmonary
nodules. In univariate logistic regression analysis, renal tumor
size (HR=1.02; 95% CI, 1.00–1.04; P=0.0356), albumin (HR=0.12; 95%
CI, 0.02–0.46; P=0.0046), pTstage (HR=11.89; 95% CI, 3.04–55.33;
P=0.0007) and renal fat invasion (HR=11.14; 95% CI, 2.39–63.86;
P=0.0032) were significantly associated with pulmonary metastasis.
In multivariate logistic regression analysis, pTstage was the only
statistically significant factor for pulmonary metastasis (HR=9.81;
95% CI, 2.29–51.30; P=0.0033). No other significant differences in
the remaining variables were indicated between groups (Table III).
| Table III.Prognostic indicators for progression
to pulmonary metastasis in patients with renal cell carcinoma with
pulmonary nodule. |
Table III.
Prognostic indicators for progression
to pulmonary metastasis in patients with renal cell carcinoma with
pulmonary nodule.
|
| Univariate
analysis | Multivariate
analysis |
|---|
|
|
|
|
|---|
| Factors | P-value | HR | 95% CI | P-value | HR | 95% CI |
|---|
| Age | 0.1839 | 1.04 | 0.98–1.11 |
|
|
|
| Renal tumor
size | 0.0356 | 1.02 | 1.00–1.04 |
|
|
|
| Renal vein
thrombus | 0.1394 | 3.67 | 0.61–22.15 |
|
|
|
| Albumin | 0.0046 | 0.12 | 0.02–0.46 | 0.0781 | 0.20 | 0.03–1.14 |
|
1pTstage | 0.0007 | 11.89 | 3.04–55.33 | 0.0033 | 9.81 | 2.29–51.30 |
| Renal fat
invasion | 0.0032 | 11.14 | 2.39–63.86 |
|
|
|
Discussion
In the present study, 62/356 patients (17.4%) with
RCC exhibited pulmonary nodules, and 15/62 patients (24.2%)
progressed to pulmonary metastasis. The prevalence of progression
to pulmonary metastasis was significantly increased in patients
with pulmonary nodules, compared with patients without pulmonary
nodules. In multivariate analysis, the presence of pulmonary
nodules was an independent prognostic factor for pulmonary
metastasis and was associated with adverse effects associated with
progression to pulmonary metastasis. Among patients with pulmonary
nodules, progression to pulmonary metastasis occurred at a
>3-fold increased rate, compared with patients without pulmonary
nodules. Taking the aforementioned into consideration, pulmonary
nodules in patients with RCC are indicated to be prognostic
indicators of pulmonary metastasis. Even though pulmonary nodules
were a significant factor in progression to pulmonary metastasis,
when preoperative pulmonary nodules are detected, no clinical
management strategy has been developed, to the best of our
knowledge, until now (13). A number
of previous studies have indicated that larger kidney tumors, renal
vein thrombus, lymph node vascular invasion and renal fat invasion
increase the adverse effects of cancer and poor prognosis by
increasing the likelihood of malignancy or recurrence (14–16).
Additionally, there are significant risk factors associated with
the presence of pulmonary nodules, the pathologic tumor stage and
tumor grade, which can be used to predict a poor prognosis
(17–19). These factors were statistically
significant in univariate analysis in the present study, but
pulmonary nodules were the most statistically significant factor in
multivariate analysis.
In the present study's subgroup analysis, including
pulmonary nodules, it was indicated that renal tumor size, albumin
level, pTstage and renal fat invasion were significantly associated
with pulmonary metastasis in univariate analyses. Chen et al
(20) reported that albumin is an
important prognostic indicator in patients with RCC, regardless of
tumor type (localized or metastatic). Cancer is frequently
accompanied by malnutrition and chronic inflammation, and albumin
levels are associated with the degree of malnutrition or
inflammatory response (21,22).
Furthermore, pTstage was a significant prognostic
indicator, consistent with previous reports (17,18). In
multivariate analyses, pTstage was the only independent prognostic
indicator for pulmonary metastasis. The size (median size >5 mm)
and number (median number >4) of pulmonary nodules have been
reported to be increased in patients with pulmonary metastasis
compared with patients with no pulmonary metastasis (13,23).
However, the size, number, site and location of pulmonary nodules
were not associated with pulmonary metastasis in the present study.
Therefore, the presence of a pulmonary nodule is a strong
prognostic indicator for pulmonary metastasis in patients with RCC.
Additionally, in patients with pulmonary nodules, pTstage was a
good prognostic indicator for pulmonary metastasis. Nevertheless,
recent guidelines for follow-up imaging (chest and radiography) by
CT or X-ray of patients who underwent radical or partial
nephrectomy (24) are based on the
pathological tumor stage. Additionally, there are no definite
guidelines for patients with pulmonary nodules (25). Therefore, the present study indicates
that the presence of pulmonary nodules may be considered as an
associated risk factor for chest radiological imaging follow-up,
particularly in patients who underwent radical or partial
nephrectomy. Additionally, follow-up imaging (chest and
radiography) by CT or X-ray should be performed more frequently,
compared with the Fleischner Society guidelines (12). Evidently, short-term follow-up imaging
may not be necessary for patients who have not been diagnosed with
RCC. Benjamin et al (26)
reported that the malignancy rate in small nodules in patients
without a known malignant tumor may be as low as 1%.
There are numerous strengths in the present study.
Firstly, the present study presents a large number of registered
patients compared with other reports (13,19), which
could reduce selection bias. Secondly, a more extensive analysis of
patient data, compared with other reports (3,10,23), was conducted by examining various
factors from the patient's history to blood test, preoperative
imaging and postoperative pathology results, including
hypertension, renal tumor site and location, pulmonary nodule
number, site and location, and serum K level. Thirdly, in another
study, the nodule was diagnosed by chest CT or X-ray and follow-up
(13,19), in contrast to the present study where
patients were diagnosed and followed up by chest CT. However, the
present study does present a number of limitations. Firstly, it was
a retrospective analysis at a single center; therefore, selection
bias may have affected the progression to pulmonary metastasis.
Secondly, the precise time that the pulmonary nodules changed to
malignant tumors could not be confirmed, due to the postoperative
chest CT imaging follow-ups not being consistent. Nevertheless, the
fact that the presence of pulmonary nodules is associated with
progression to pulmonary metastasis is of notable value, as they
may be stronger risk factors, compared with other preoperative
factors. The presence of pulmonary nodules is an important
prognostic indicator to consider in the diagnosis and management of
patients with RCC.
In conclusion, in patients with RCC who underwent
radical or partial nephrectomy, patients with pulmonary nodules had
a significantly increased probability of progression to pulmonary
metastasis, compared with patients without pulmonary nodules.
Additionally, in patients with pulmonary nodules, pTstage was
significantly associated with progression to pulmonary metastasis.
Further studies involving a more aggressive short-term chest
radiography follow-up are required for patients with RCC with
pulmonary nodules or higher pTstages.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
JYK, JGL and HKH analyzed the data and contributed
to the conception and design of the present study. JYK, JGL, CHL
and SHC assisted in the acquisition, analysis and interpretation of
data. CHL, HKH and SHC were involved in drafting the manuscript and
revising it critically for intellectual content. SK and SBH
confirmed the preoperative and postoperative chest CT. HKH and SHC
gave final approval for the publication of the final version of the
manuscript following overall revision. All authors have read and
approved the final version of the manuscript.
Ethics approval and consent to
participate
The present study was appoved by the Pusan National
University Hospital Institutional Review Board (approval no.
1802-004-063). Written informed consent was obtained from all
patients prior to enrollment in the study.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Kummerlin IP, ten Kate FJ, Wijkstra H, de
la Rosette JJ and Laguna MP: Changes in the stage and surgical
management of renal tumours during 1995–2005: An analysis of the
Dutch national histopathology registry. BJU Int. 102:946–951. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Chang JS, Park YH, Ku JH, Kwak C and Kim
HH: Predicting factors for death from other causes in patients with
localized renal cell carcinoma. Korean J Urol. 53:18–22. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Mano R, Vertosick E, Sankin AI, Chevinsky
MS, Larish Y, Jakubowski CD, Hötker AM, Hakimi AA, Sjoberg DD, Akin
O and Russo P: Subcentimeter pulmonary nodules are not associated
with disease progression in patients with renal cell carcinoma. J
Urol. 193:776–82. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Ljungberg B: The role of metastasectomy in
renal cell carcinoma in the era of targeted therapy. Curr Urol Rep.
14:19–25. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Bianchi M, Sun M, Jeldres C, Shariat SF,
Trinh QD, Briganti A, Tian Z, Schmitges J, Graefen M, Perrotte P,
et al: Distribution of metastatic sites in renal cell carcinoma: A
population-based analysis. Ann Oncol. 23:973–980. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Ueda K, Suekane S, Mitani T, Chikui K,
Ejima K, Suyama S, Nakiri M, Nishihara K, Matsuo M and Igawa T:
Spontaneous regression of multiple pulmonary nodules in a patient
with unclassified renal cell carcinoma following laparoscopic
partial nephrectomy: A case report 5. Mol Clin Oncol. 5:49–52.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Phua CK, Sim WY, Sen Tee K, Lew SJ, Lim
AY, Tai DY, Goh SK, Kor AC, Ng AW, Abisheganaden J and Verma A:
Evaluation of pulmonary nodules in Asian population. J Thorac Dis.
8:950–957. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Field JK, Marcus MW and Oudkerk M: Risk
assessment in relation to the detection of small pulmonary nodules.
Transl Lung Cancer Res. 6:35–41. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Griffin N, Gore ME and Sohaib SA: Imaging
in metastatic renal cell carcinoma. AJR Am J Roentgenol.
189:360–370. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Khokhar S, Vickers A, Moore MS, Mironov S,
Stover DE and Feinstein MB: Significance of non-calcified pulmonary
nodules in patients with extrapulmonary cancers. Thorax.
61:331–336. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Donat SM, Diaz M, Bishoff JT, Coleman JA,
Dahm P, Derweesh IH, Herrell SD III, Hilton S, Jonasch E, Lin DW,
et al: Follow-up for clinically localized renal neoplasms: AUA
Guideline. J Urol. 190:407–16. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
MacMahon H, Austin JH, Gamsu G, Herold CJ,
Jett JR, Naidich DP, Patz EF Jr and Swensen SJ: Fleischner Society:
Guidelines for management of small pulmonary nodules detected on CT
scans: A statement from the Fleischner Society. Radiology.
237:395–400. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Adibi M, Kenney PA, Thomas AZ, Borregales
LD, Nogueras-Gonzalez GM, Wang X, Devine CE, Karam JA and Wood CG:
Prediction of pulmonary metastasis in renal cell carcinoma patients
with indeterminate pulmonary nodules. Eur Urol. 69:352–360. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Mouracade P, Kara O, Maurice MJ, Dagenais
J, Malkoc E, Nelson RJ and Kaouk JH: Patterns and predictors of
recurrence after partial nephrectomy for kidney tumors. J Urol.
197:1403–1409. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Katz MD, Serrano MF, Humphrey PA, Grubb RL
III, Skolarus TA, Gao F and Kibel AS: The role of lymphovascular
space invasion in renal cell carcinoma as a prognostic marker of
survival after curative resection. Urol Oncol. 29:738–744. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Abel EJ, Margulis V, Bauman TM, Karam JA,
Christensen WP, Krabbe LM, Haddad A, Golla V and Wood CG: Risk
factors for recurrence after surgery in non-metastatic RCC with
thrombus: A contemporary multicentre analysis. BJU Int.
117:E87–E94. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Adamy A, Chong KT, Chade D, Costaras J,
Russo G, Kaag MG, Bernstein M, Motzer RJ and Russo P: Clinical
characteristics and outcomes of patients with recurrence 5 years
after nephrectomy for localized renal cell carcinoma. J Urol.
185:433–438. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Sun M, Shariat SF, Cheng C, Ficarra V,
Murai M, Oudard S, Pantuck AJ, Zigeuner R and Karakiewicz PI:
Prognostic factors and predictive models in renal cell carcinoma: A
contemporary review. Eur Urol. 60:644–661. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Xu R, Horick N, McGovern FJ, Dahl DM,
Feldman AS, Blute ML, Olumi AF and Michaelson MD: Prognostic
significance of indeterminate lung nodules in renal cell carcinoma.
Urol Oncol. 32:355–361. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Chen Z, Shao Y, Wang K, Cao W, Xiong Y, Wu
R, Luo S, Xu X and He X: Prognostic role of pretreatment serum
albumin in renal cell carcinoma: A systematic review and
meta-analysis. Onco Targets Ther. 9:6701–6710. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Bauer J and Capra S: Comparison of a
malnutrition screening tool with subjective global assessment in
hospitalised patients with cancer-sensitivity and specificity. Asia
Pac J Clin Nutr. 12:257–260. 2003.PubMed/NCBI
|
|
22
|
McMillan DC, Watson WS, O'Gorman P,
Preston T, Scott HR and McArdle CS: Albumin concentrations are
primarily determined by the body cell mass and the systemic
inflammatory response in cancer patients with weight loss. Nutr
Cancer. 39:210–213. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Henschke CI, Yankelevitz DF, Naidich DP,
McCauley DI, McGuinness G, Libby DM, Smith JP, Pasmantier MW and
Miettinen OS: CT screening for lung cancer: Suspiciousness of
nodules according to size on baseline scans. Radiology.
231:164–168. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Gould MK, Fletcher J, Iannettoni MD, Lynch
WR, Midthun DE, Naidich DP and Ost DE: American College of Chest
Physicians: Evaluation of patients with pulmonary nodules: When is
it lung cancer? ACCP evidence-based clinical practice guidelines
(2nd edition). Chest. 132 (3 Suppl):108S–130S. 2007.
|
|
25
|
Callister ME and Baldwin DR: How should
pulmonary nodules be optimally investigated and managed? Lung
Cancer. 91:48–55. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Benjamin MS, Drucker EA, McLoud TC and
Shepard JA: Small pulmonary nodules: Detection at chest CT and
outcome. Radiology. 226:489–493. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Sobin LH, Gospodariwicz M and Wittekind C:
TNM classification of malignant tumors. UICC International Union
Against Cancer. 7th. Wiley-Blackwell; pp. 2552009
|