Introduction
Stomach cancer accounts for over 1,000,000 cases
annually worldwide. It is the fourth leading cause of cancer and
the fifth leading cause of mortality (1). Recent studies show that the five-year
overall survival (OS) of patients undergoing endoscopic resection
or laparoscopy-assisted distal gastrectomy for gastric cancer is
89.0-98.2% (2,3). However, the long-term outcomes of
patients with advanced or unresectable gastric cancer remain poor.
Despite recent advances in chemotherapeutics, the median OS was
reported to be 13.1-17.45 months when patients with unresectable
advanced gastric cancer received immunotherapy plus chemotherapy
(4,5).
A study from the Netherlands reported a median OS of
four months in gastric cancer patients with peritoneal metastasis
(6). Intraperitoneal paclitaxel, in
addition to systemic chemotherapy, was developed to improve their
outcomes; however, the median OS in patients undergoing
intraperitoneal paclitaxel with systemic chemotherapy was not found
superior to that of patients undergoing systemic chemotherapy alone
(17.7 months vs. 15.2 months, P=0.08) in the PHOENIX-GC trial
(7). In clinical settings, the
presence of massive ascites can impair activities of daily living,
resulting in poor prognosis. Additionally, many clinical trials
exclude gastric cancer patients with massive ascites caused by
peritoneal metastasis, suggesting that data from clinical studies
may not reflect the clinical course of patients with peritoneal
metastasis.
Therefore, this study aimed to examine whether the
presence or degree of ascites in advanced gastric cancer influenced
prognostic value using real-world data.
Patients and methods
Patients
We retrospectively included 124 advanced gastric
cancer patients who were diagnosed or treated at Fukuchiyama City
Hospital from April 2009 to March 2020. We assessed patient
characteristics, including blood chemical analysis at diagnosis,
age, sex, and Eastern Cooperative Oncology Group Performance Status
(ECOG-PS). We also assessed clinicopathological characteristics
such as macroscopic type, location, histological type, human
epidermal growth factor receptor 2 (HER2) status, liver metastasis,
bone metastasis, and the presence and degree of ascites. The
histological type was classified as intestinal or diffuse type
according to the Lauren classification (8). Blood chemical analysis included the
following items: white blood cell count, hemoglobin, platelet
count, total protein, albumin, alkaline phosphatase (ALP), lactate
dehydrogenase (LDH), C-reactive protein (CRP), carcinoembryonic
antigen (CEA), carbohydrate antigen 19-9 (CA19-9) and
neutrophil-to-lymphocyte ratio (NLR). We also assessed psoas muscle
mass index (PMI) as a sarcopenia index (9). The calculation of PMI was performed as
described previously (10). We also
collected the data on the treatment and chemotherapy regimens. This
study was conducted in accordance with the Declaration of Helsinki
and approved by the Ethics Committee of Fukuchiyama City Hospital
(approval no. 2-64). An opt-out method was conducted to obtain
informed consent because this was a retrospective study.
Assessment of ascites and overall
survival
The degree of ascites was assessed using computed
tomography at diagnosis and classified as none, small (within the
pelvic cavity), moderate (beyond the pelvic cavity), or massive
(extending throughout the abdominal cavity), based on the
classification used in previous studies (Fig. 1) (7,11,12).
The overall survival (OS) rate was evaluated from the date of
computed tomography examination to the last follow-up date or date
of death. We compared the OS to the presence or amount of
ascites.
Uni- and multivariate Cox proportional hazards
analyses were conducted to identify predictors of OS in patients
with advanced gastric cancer. The variables included age, sex,
ECOG-PS, macroscopic type, histological type, HER2 status, liver
metastasis, bone metastasis, ascites, moderate or massive ascites,
ALP, LDH, CEA, CA19-9, NLR, PMI, and chemotherapy. The cut-off
values for ALP, LDH, CEA, and CA19-9 were defined using the upper
limit of the normal ranges. The cut-off values for PMI were defined
using medians in the male and female (10). We compared the clinical features of
patients with moderate or massive ascites and those without
moderate or massive ascites.
Statistical analysis
Statistical analysis was performed using the IBM
SPSS Statistics 27 (IBM Japan, Tokyo, Japan) or R version 4.3.2 (R
Foundation for Statistical Computing, Vienna, Austria). Statistical
significance was set at P<0.05. Continuous variables are
presented as medians and ranges, and comparisons were conducted
using the Mann-Whitney U test. Categorical variables are expressed
as numbers and percentages, and comparisons were performed using
the χ2 test or Fisher's exact test. The OS rate was
evaluated using Kaplan-Meier survival curves and the log-rank
tests. Cox proportional hazards model analysis was used to estimate
hazard ratio (HR) and 95% confidence interval (CI). Significant
variables in the univariate analysis were included in the
multivariate analysis.
Results
Clinicopathological characteristics of
advanced gastric cancer
Table I presents the
clinicopathological characteristics. The median age was 73, and the
proportion of males was 66.9%. The median follow-up period was
232.5 days, and 112 patients (90.3%) died. The ratio of Borrmann
type III or IV in the macroscopic type was 51.6%. Regarding the
histological type, the percentage of the intestinal type was 45.2%,
while that of the diffuse type was 53.2%. In this study, 43.5% of
the patients had ascites of whom 20.2% had moderate or massive
ascites. The median PMI was 4.69 in males, and 3.39 in females.
 | Table I.Clinicopathological characteristics of
patients with advanced gastric cancer. |
Table I.
Clinicopathological characteristics of
patients with advanced gastric cancer.
| Characteristic | Value |
|---|
| Median age, years
(range) | 73 (31–97) |
| Sex, n (%) |
|
|
Female | 41 (33.1) |
| Male | 83 (66.9) |
| ECOG-PS, n (%) |
|
| 0 or
1 | 96 (77.4) |
| 2 or
above | 27 (21.8) |
|
Unknown | 1 (0.8) |
| Median follow-up
period, days (range) | 232.5 (5–2,656) |
| Deaths during
follow-up period, n (%) | 112 (90.3) |
| Macroscopic type, n
(%) |
|
| Borrmann
type III or IV | 64 (51.6) |
|
Others | 60 (48.4) |
| Location, n (%) |
|
|
Upper | 40 (32.3) |
|
Middle | 43 (34.7) |
|
Lower | 41 (33.1) |
| Histological type, n
(%) |
|
|
Intestinal | 56 (45.2) |
|
Diffuse | 66 (53.2) |
|
Others | 2 (1.6) |
| HER2 status, n
(%) |
|
|
Negative | 71 (57.3) |
|
Positive | 10 (8.1) |
|
Unknown | 43 (34.7) |
| Liver metastasis, n
(%) |
|
|
Absent | 74 (59.7) |
|
Present | 50 (40.3) |
| Bone metastasis, n
(%) |
|
|
Absent | 119 (96.0) |
|
Present | 5 (4.0) |
| Ascites, n (%) |
|
|
Absent | 70 (56.5) |
|
Present | 54 (43.5) |
| Moderate or massive
ascites, n (%) |
|
|
Absent | 99 (79.8) |
|
Present | 25 (20.2) |
| PMI,
cm2/m2 (range) |
|
|
Male | 4.69
(1.98-8.40) |
|
Female | 3.39
(1.22-5.41) |
Table II presents
the laboratory findings and treatment pattern of patients with
advanced gastric cancer. Regarding tumor markers, the median CEA
level was 5.4 ng/ml, whereas the median CA19-9 level was 34.6
ng/ml. For the inflammatory markers, the median NLR was 3.91.
Regarding treatment, 40 patients (32.3%) received best supportive
care, 84 (67.7%) underwent chemotherapy. As for the first-line
chemotherapy regimen, 38 (30.6%) patients received cisplatin-based
chemotherapy, 30 (24.2%) received oxaliplatin-based chemotherapy, 9
(7.3%) received fluoropyrimidine monotherapy, 5 (4.0%) received
taxane-based chemotherapy, while 2 (1.6%) did in other
institutions.
| Table II.Laboratory findings and treatment in
advanced gastric cancer patients. |
Table II.
Laboratory findings and treatment in
advanced gastric cancer patients.
| Laboratory findings
and treatment pattern | Value |
|---|
| Laboratory
findings, median (range) |
|
| White
blood cell, /µl | 7,025
(3,560–47,500) |
|
Hemoglobin, g/dl | 10.75
(3.5-17.8) |
|
Platelet,
104/µl | 26.6
(11.8-69.6) |
| Total
protein, g/dl | 6.4 (4.6-8.5) |
|
Albumin, g/dl | 3.4 (1.9-4.5) |
| ALP,
IU/l | 267
(116–3,186) |
| LDH,
IU/l | 202.5
(122–1,266) |
| CRP,
mg/dl | 1.15
(0.01-36.9) |
| CEA,
ng/ml | 5.4
(0.7-7,827.1) |
| CA19-9,
U/ml | 34.6
(2.0-120,000) |
|
NLR | 3.91
(1.20-36.69) |
| Treatment, n
(%) |
|
| Best
supportive care | 40 (32.3) |
|
First-line chemotherapy | 84 (67.7) |
|
Cisplatin-based
chemotherapy | 38 (30.6) |
|
Oxaliplatin-based
chemotherapy | 30 (24.2) |
|
Fluoropyrimidine
monotherapy | 9 (7.3) |
|
Taxane-based
chemotherapy | 5 (4.0) |
|
Unknown | 2 (1.6) |
Clinical outcomes with respect to
ascites
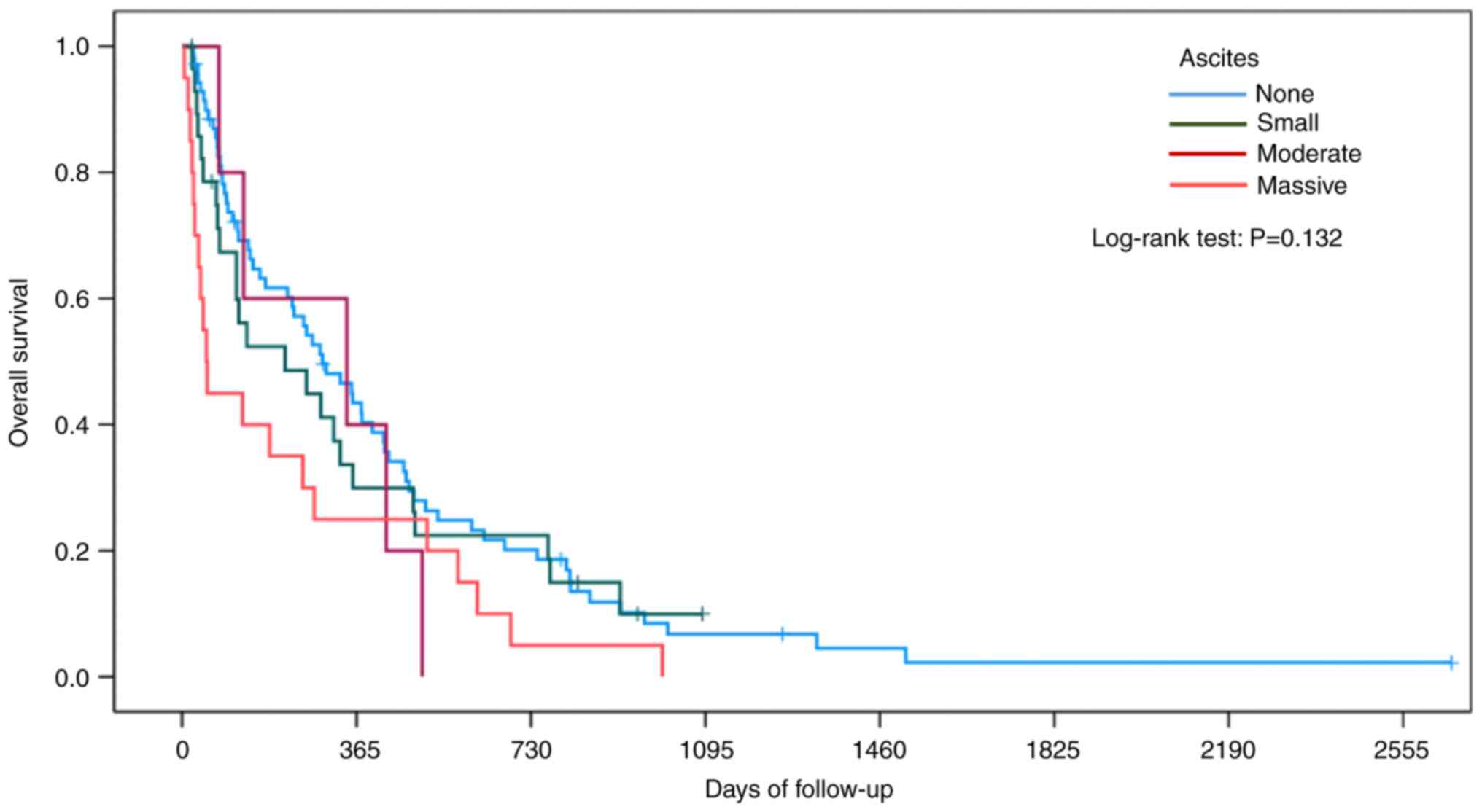
Fig. 2 shows the OS
according to the staging of ascites. The median OS was 294.0 days
(95% CI, 182.0-406.0 days) in patients without ascites, 216.0 days
(95% CI, 0.0-454.3 days) in patients with small ascites, 345.0 days
(95% CI, 0.0-808.8 days) in patients with moderate ascites, and
51.0 days (95% CI, 31.3-70.7 days) in patients with massive ascites
(P=0.132).
Fig. 3A shows the OS
based on the presence of ascites. The median OS was 294.0 days (95%
CI, 182.0-406.0 days) in patients without ascites, and 136.0 days
(95% CI, 17.3-254.7 days) in patients with ascites (P=0.116). The
cumulative one-year, and two-year OS rates in patients without
ascites were 43.5 and 20.2%, respectively, whereas those in
patients with ascites were 29.1 and 13.6%, respectively. Fig. 3B shows the OS according to moderate
or massive ascites. The median OS was 289.0 days (95% CI,
204.0-374.0 days) in patients without moderate or massive ascites,
and 127.0 days (95% CI, 3.0-251.0 days) in patients with moderate
or massive ascites (P=0.027). The cumulative one-year, and two-year
OS rates in patients without moderate or massive ascites were 39.5
and 20.9%, respectively, whereas those in patients with moderate or
massive ascites were 28.0 and 4.0%, respectively.
Predictors of overall survival in
patients with advanced gastric cancer
Table III shows
the predictors of OS in patients with advanced gastric cancer. In
univariate analysis, age ≥80 (HR, 2.243; 95% CI, 1.503-3.347;
P<0.001), ECOG-PS ≥2 (HR, 3.277; 95% CI, 2.049-5.238;
P<0.001), diffuse type (HR, 1.551; 95% CI, 1.051-2.289;
P=0.027), moderate or massive ascites (HR, 1.650; 95% CI,
1.053-2.586; P=0.029), ALP >321 (HR, 1.569; 95% CI, 1.053-2.336;
P=0.027), LDH >245 (HR, 1.535; 95% CI, 1.039-2.267; P=0.031),
NLR >5 (HR, 2.187; 95% CI, 1.479-3.232; P<0.001), and
chemotherapy (HR, 0.145; 95% CI, 0.091-0.231; P<0.001) were
determined to be predictive factors. In multivariate analysis,
diffuse type (HR, 1.532; 95% CI, 1.002-2.343; P=0.049), moderate or
massive ascites (HR, 2.153; 95% CI, 1.301-3.564; P=0.003), and
chemotherapy (HR, 0.189; 95% CI, 0.101-0.352; P<0.001) were
significant predictive factors for OS.
| Table III.Predictors of overall survival in
patients with advanced gastric cancer. |
Table III.
Predictors of overall survival in
patients with advanced gastric cancer.
|
| Univariate
analysis | Multivariate
analysis |
|---|
|
|
|
|
|---|
| Characteristic | HR | 95% CI | P-value | HR | 95% CI | P-value |
|---|
| Age, years |
|
|
|
|
|
|
| 80 or
above | 2.243 | 1.503-3.347 | <0.001 | 1.387 | 0.817-2.353 | 0.226 |
| Sex |
|
|
|
|
|
|
|
Male | 0.775 | 0.524-1.145 | 0.200 |
|
|
|
| ECOG-PS |
|
|
|
|
|
|
| 2 or
above | 3.277 | 2.049-5.238 | <0.001 | 1.661 | 0.987-2.797 | 0.056 |
| Macroscopic
type |
|
|
|
|
|
|
|
Borrmann type III or IV | 1.387 | 0.952-2.022 | 0.089 |
|
|
|
| Histological
type |
|
|
|
|
|
|
|
Diffuse | 1.551 | 1.051-2.289 | 0.027 | 1.532 | 1.002-2.343 | 0.049 |
| HER2 status |
|
|
|
|
|
|
|
Positive | 0.961 | 0.490-1.885 | 0.909 |
|
|
|
| Liver
metastasis |
|
|
|
|
|
|
|
Present | 0.951 | 0.647-1.396 | 0.796 |
|
|
|
| Bone
metastasis |
|
|
|
|
|
|
|
Present | 2.250 | 0.894-5.663 | 0.085 |
|
|
|
| Ascites |
|
|
|
|
|
|
|
Present | 1.351 | 0.926-1.969 | 0.118 |
|
|
|
| Moderate or massive
ascites |
|
|
|
|
|
|
|
Present | 1.650 | 1.053-2.586 | 0.029 | 2.153 | 1.301-3.564 | 0.003 |
| ALP, IU/l |
|
|
|
|
|
|
|
>321 | 1.569 | 1.053-2.336 | 0.027 | 1.722 | 0.984-3.015 | 0.057 |
| LDH, IU/l |
|
|
|
|
|
|
|
>245 | 1.535 | 1.039-2.267 | 0.031 | 1.184 | 0.716-1.957 | 0.511 |
| CEA, ng/ml |
|
|
|
|
|
|
|
>5 | 1.001 | 0.676-1.483 | 0.996 |
|
|
|
| CA19-9, U/ml |
|
|
|
|
|
|
|
>37 | 1.072 | 0.722-1.593 | 0.729 |
|
|
|
| NLR |
|
|
|
|
|
|
|
>5 | 2.187 | 1.479-3.232 | <0.001 | 1.338 | 0.863-2.074 | 0.194 |
| PMI |
|
|
|
|
|
|
|
Low | 1.234 | 0.849-1.793 | 0.271 |
|
|
|
| Chemotherapy |
|
|
|
|
|
|
|
Present | 0.145 | 0.091-0.231 | <0.001 | 0.189 | 0.101-0.352 | <0.001 |
Clinical features of patients with
moderate or massive ascites and those without moderate or massive
ascites
Table IV shows
comparative clinical features between patients with moderate or
massive ascites and those without it. Gastric cancer showing
Borrmann type III or IV was significantly higher in those with
moderate or massive ascites compared with those without moderate or
massive ascites (76.0% vs. 45.5%, P=0.012). In contrast, no
significant differences were observed regarding age, sex, ECOG-PS,
tumor location, histological type, and HER2 status. Regarding
laboratory findings, hemoglobin concentration was significantly
higher in the patients with moderate or massive ascites than those
without moderate or massive ascites (12.3 g/dl vs. 10.4 g/dl,
P=0.020). Furthermore, the serum CEA level was significantly lower
in patients with moderate or massive ascites than those without
moderate or massive ascites (3.4 ng/dl vs. 7.3 ng/dl, P=0.020). As
for chemotherapy, the presence or absence of treatment with first-
and second-line chemotherapy was not significantly different.
| Table IV.Clinical features of patients with
moderate or massive ascites and those without moderate or massive
ascites. |
Table IV.
Clinical features of patients with
moderate or massive ascites and those without moderate or massive
ascites.
| Characteristic | Patients without
moderate or massive ascites | Patients with
moderate or massive ascites | P-value |
|---|
| Median age, years
(range) | 73 (31–97) | 72 (31–90) | 0.527 |
| Sex, n (%) |
|
| 0.911 |
|
Female | 32 (32.3) | 9 (36.0) |
|
|
Male | 67 (67.7) | 16 (64.0) |
|
| ECOG-PS, n
(%)a |
|
| 0.584 |
| 0 or
1 | 78 (79.6) | 18 (72.0) |
|
| 2 or
above | 20 (20.4) | 7 (28.0) |
|
| Macroscopic type, n
(%) |
|
| 0.012 |
|
Borrmann type III or IV | 45 (45.5) | 19 (76.0) |
|
|
Others | 54 (54.5) | 6 (24.0) |
|
| Location, n
(%) |
|
| 0.336 |
|
Upper | 29 (29.3) | 11 (44.0) |
|
|
Middle | 35 (35.4) | 8 (32.0) |
|
|
Lower | 35 (35.4) | 6 (24.0) |
|
| Histological type,
n (%)b |
|
| 0.108 |
|
Intestinal | 49 (50.0) | 7 (29.2) |
|
|
Diffuse | 49 (50.0) | 17 (70.8) |
|
| HER2 status, n
(%)c |
|
| 1.000 |
|
Negative | 58 (87.9) | 13 (86.7) |
|
|
Positive | 8 (12.1) | 2 (13.3) |
|
| Laboratory
findings, median (range) |
|
|
|
| White
blood cell, /µl | 6,840
(3,560–47,500) | 7,770
(4,140–14,750) | 0.130 |
|
Hemoglobin, g/dl | 10.4
(3.5-17.8) | 12.3
(5.4-17.2) | 0.020 |
|
Platelet,
104/µl | 26.0
(11.8-69.6) | 27.3
(12.4-67.0) | 0.711 |
| Total
protein, g/dl | 6.4 (4.6-8.5) | 6.5 (5.2-7.9) | 0.165 |
|
Albumin, g/dl | 3.4 (1.9-4.5) | 3.2 (1.9-4.5) | 0.456 |
| ALP,
IU/l | 280
(118–3,186) | 253
(116–3,124) | 0.581 |
| LDH,
IU/l | 202
(122–1,266) | 203 (156–831) | 0.560 |
| CRP,
mg/dl | 0.69
(0.01-18.51) | 2.63
(0.01-36.90) | 0.073 |
| CEA,
ng/ml | 7.3
(0.7-7,827.1) | 3.4
(0.7-6,816.0) | 0.019 |
| CA19-9,
U/ml | 36.85
(2.0-120,000) | 24.5
(2.1-5,1486.7) | 0.908 |
|
NLR | 3.6 (1.2-36.7) | 6.0 (1.2-29.4) | 0.054 |
| First-line
chemotherapy, n (%) |
|
| 0.835 |
|
Absent | 31 (31.3) | 9 (36.0) |
|
|
Present | 68 (68.7) | 16 (64.0) |
|
| Second-line
chemotherapy, n (%)d |
|
| 1.000 |
|
Absent | 18 (28.6) | 5 (31.3) |
|
|
Present | 45 (71.4) | 11 (68.8) |
|
| PMI, n
(%)e |
|
| 0.178 |
|
High | 52 (53.6) | 9 (36.0) |
|
|
Low | 45 (46.4) | 16 (64.0) |
|
Discussion
In this study, we assessed clinicopathological
factors, including the degree of ascites, to determine predictive
factors in patients with advanced gastric cancer. The OS of
patients with moderate or massive ascites was significantly lower
than that of patients without moderate or massive ascites.
Furthermore, multivariate analysis revealed that diffuse type,
moderate or massive ascites, and chemotherapy were pivotal
prognostic factors for OS. Collectively, we observed that moderate
or massive ascites could influence OS in patients with advanced
gastric cancer in a clinical setting.
Previous studies have shown that the presence of
ascites or peritoneal metastases is a pivotal prognostic factor in
patients with advanced gastric cancer who are undergoing
chemotherapy (13–15). A prognostic index consisting of the
ECOG-PS, number of metastatic sites, prior gastrectomy, and serum
ALP level has been established and validated in advanced gastric
cancer using phase III study data (16,17).
In clinical settings, patients with advanced gastric cancer who
occasionally present with massive ascites cannot receive systemic
chemotherapy because of impaired activities of daily living or
inadequate oral intake. Absence of chemotherapy, in addition to
malignant ascites itself, may worsen the outcomes of such patients.
Accordingly, we aimed to evaluate the prognostic factors of
advanced gastric cancer, including patients who did not receive
chemotherapy.
We determined that age ≥80, ECOG-PS ≥2, diffuse
type, moderate or massive ascites, elevated ALP, elevated LDH,
elevated NLR, and no chemotherapy were poor prognostic factors in
the univariate analysis. Prognostic scoring models in advanced
gastric cancer have revealed that malignant ascites and peritoneal
metastasis are critical parameters for predicting OS (13–15,18).
In contrast, another study showed that peritoneal metastasis is not
associated with OS (16). The study
used the clinical trial data, in which patients with ascites beyond
the pelvic cavity were excluded (19). This may explain why peritoneal
metastasis could not influence OS in the study. However, we
encountered patients with abdominal distention due to ascites in
the clinical setting. Indeed, 20.2% of patients in this study
presented with moderate or massive ascites. Our results imply that
that moderate or massive ascites could be a more effective
prognostic factor than ascites alone. For serum indicators, serum
ALP level has been reported to be a predictive factor of OS in
previous studies (13–17,20),
and serum LDH level was also a prognostic factor in some studies
(18,20). The NLR, an inflammatory biomarker,
has been recognized as a prognostic factor for solid tumors,
including gastric cancer (20–23).
Collectively, our data suggest that ALP, LDH, and NLR may influence
OS in patients with advanced gastric cancer, as previously
reported.
Diffuse type, moderate or excessive ascites, and
chemotherapy were the pivotal prognostic factors in multivariate
analysis. These findings imply that moderate or massive ascites at
diagnosis could influence the OS in patients with advanced gastric
cancer.
In this study, the ECOG-PS, or the ratio of patients
undergoing first- and second-line chemotherapy did not differ
between patients with moderate or massive ascites and those without
moderate or massive ascites. In contrast, the NLR and CRP levels
tended to be higher in patients with moderate or massive ascites,
suggesting carcinomatous peritonitis. Collectively, the poor OS in
patients with moderate or massive ascites may be due to systemic
inflammation caused by carcinomatous peritonitis. In addition, we
determined that the proportion of the macroscopic type showing
Borrmann type III or IV was higher in patients with moderate or
massive ascites. A previous study revealed that macroscopic type
III or IV was pivotal in detecting peritoneal metastases in gastric
cancer (24). These findings imply
that the macroscopic type was associated with peritoneal
metastases. Hemoglobin concentration was significantly higher in
the patients with moderate or massive ascites. This finding
suggests that intravascular dehydration might occur in patients
with moderate or massive ascites. Furthermore, the serum CEA level
was significantly lower in patients with moderate or massive
ascites. The reason for the difference remains unknown. However,
the sensitivity of CEA for peritoneal metastasis was 19% (25). Thus, the serum CEA level may not
reflect malignant ascites or peritoneal metastasis.
This study had some limitations. First, this was
conducted at a single center with a retrospective design; thus, a
multicenter prospective study is needed to ascertain our findings.
Second, our study included 124 advanced gastric cancer patients. It
is difficult to generalize our findings due to the small number of
patients. Third, all cases with ascites were not proven to have
peritoneal metastases on histological examination. Indeed,
peritoneal metastases were not confirmed by histological
examinations in five of 25 cases showing moderate or excessive
ascites, although peritoneal metastases were clinically diagnosed.
Fourth, only Japanese patients with advanced gastric cancer were
registered. Therefore, these results should be validated in other
populations.
Using real-world data, our study determined that
moderate or massive ascites at diagnosis could influence OS in
advanced gastric cancer.
Acknowledgements
Not applicable.
Funding
This work was supported by a Grant-in-Aid for Early-Career
Scientists from the Japanese Society for the Promotion of Science
KAKENHI (grant no. 22K16051) to Naoto Iwai.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
NI, TOh, TOk, KO, HS, MKK, TTs, JS, KK, TD, KI, OD,
NY, KU, TI, TTa, HK and YI contributed to the study's conception
and design. Data collection and analysis were performed by NI, TOh,
TOk, KO, HS, MKK, TTs and JS. NI, TOh, and TOk confirm the
authenticity of all the raw data. All analyses were supervised by
KK, TD, KI, OD, NY, KU, TI, TTa, HK and YI. The first draft of the
manuscript was written by NI and all authors commented on previous
versions. All authors read and approved the final manuscript.
Ethics approval and consent to
participate
This study was conducted in accordance with the
Declaration of Helsinki and approved by the Ethics Committee of
Fukuchiyama City Hospital (approval no. 2-64). An opt-out method
was conducted to obtain informed consent because this was a
retrospective study.
Patient consent for publication
An opt-out method was conducted to obtain informed
consent.
Competing interests
All authors declare that they have no competing
interests.
References
|
1
|
Sung H, Ferlay J, Siegel RL, Laversanne M,
Soerjomataram I, Jemal A and Bray F: Global cancer statistics 2020:
GLOBOCAN estimates of incidence and mortality worldwide for 36
cancers in 185 countries. CA Cancer J Clin. 71:209–249. 2021.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Suzuki H, Ono H, Hirasawa T, Takeuchi Y,
Ishido K, Hoteya S, Yano T, Tanaka S, Toya Y, Nakagawa M, et al:
Long-term survival after endoscopic resection for gastric cancer:
Real-world evidence from a multicenter prospective cohort. Clin
Gastroenterol Hepatol. 21:307–318.e2. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Hiki N, Katai H, Mizusawa J, Nakamura K,
Nakamori M, Yoshikawa T, Kojima K, Imamoto H, Ninomiya M, Kitano S,
et al: Long-term outcomes of laparoscopy-assisted distal
gastrectomy with suprapancreatic nodal dissection for clinical
stage I gastric cancer: A multicenter phase II trial (JCOG0703).
Gastric Cancer. 21:155–161. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Janjigian YY, Shitara K, Moehler M,
Garrido M, Salman P, Shen L, Wyrwicz L, Yamaguchi K, Skoczylas T,
Campos Bragagnoli A, et al: First-line nivolumab plus chemotherapy
versus chemotherapy alone for advanced gastric, gastro-oesophageal
junction, and oesophageal adenocarcinoma (CheckMate 649): A
randomised, open-label, phase 3 trial. Lancet. 398:27–40. 2021.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Kang YK, Chen LT, Ryu MH, Oh DY, Oh SC,
Chung HC, Lee KW, Omori T, Shitara K, Sakuramoto S, et al:
Nivolumab plus chemotherapy versus placebo plus chemotherapy in
patients with HER2-negative, untreated, unresectable advanced or
recurrent gastric or gastro-oesophageal junction cancer
(ATTRACTION-4): A randomised, multicentre, double-blind,
placebo-controlled, phase 3 trial. Lancet Oncol. 23:234–247. 2022.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Thomassen I, van Gestel YR, van Ramshorst
B, Luyer MD, Bosscha K, Nienhuijs SW, Lemmens VE and de Hingh IH:
Peritoneal carcinomatosis of gastric origin: A population-based
study on incidence, survival and risk factors. Int J Cancer.
134:622–628. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Ishigami H, Fujiwara Y, Fukushima R,
Nashimoto A, Yabusaki H, Imano M, Imamoto H, Kodera Y, Uenosono Y,
Amagai K, et al: Phase III trial comparing intraperitoneal and
intravenous paclitaxel plus S-1 versus cisplatin plus S-1 in
patients with gastric cancer with peritoneal metastasis: PHOENIX-GC
trial. J Clin Oncol. 36:1922–1929. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Lauren P: THE Two Histological Main Types
Of Gastric Carcinoma: Diffuse and so-called intestinal-type
carcinoma. An attempt at a histo-clinical classification. Acta
Pathol Microbiol Scand. 64:31–49. 1965. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Okumura S, Kaido T, Hamaguchi Y, Fujimoto
Y, Masui T, Mizumoto M, Hammad A, Mori A, Takaori K and Uemoto S:
Impact of preoperative quality as well as quantity of skeletal
muscle on survival after resection of pancreatic cancer. Surgery.
157:1088–1098. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Iwai N, Okuda T, Oka K, Sakagami J, Harada
T, Ohara T, Hattori C, Taniguchi M, Sakai H, Hara T, et al:
Depletion of psoas muscle mass after systemic chemotherapy is
associated with poor prognosis in patients with unresectable
pancreatic cancer. Cancers (Basel). 13:38602021. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Nishina T, Boku N, Gotoh M, Shimada Y,
Hamamoto Y, Yasui H, Yamaguchi K, Kawai H, Nakayama N, Amagai K, et
al: Randomized phase II study of second-line chemotherapy with the
best available 5-fluorouracil regimen versus weekly administration
of paclitaxel in far advanced gastric cancer with severe peritoneal
metastases refractory to 5-fluorouracil-containing regimens
(JCOG0407). Gastric Cancer. 19:902–910. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Nakajima TE, Yamaguchi K, Boku N, Hyodo I,
Mizusawa J, Hara H, Nishina T, Sakamoto T, Shitara K, Shinozaki K,
et al: Randomized phase II/III study of 5-fluorouracil/l-leucovorin
versus 5-fluorouracil/l-leucovorin plus paclitaxel administered to
patients with severe peritoneal metastases of gastric cancer
(JCOG1108/WJOG7312G). Gastric Cancer. 23:677–688. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Chau I, Norman AR, Cunningham D, Waters
JS, Oates J and Ross PJ: Multivariate prognostic factor analysis in
locally advanced and metastatic esophago-gastric cancer-pooled
analysis from three multicenter, randomized, controlled trials
using individual patient data. J Clin Oncol. 22:2395–2403. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Lee J, Lim T, Uhm JE, Park KW, Park SH,
Lee SC, Park JO, Park YS, Lim HY, Sohn TS, et al: Prognostic model
to predict survival following first-line chemotherapy in patients
with metastatic gastric adenocarcinoma. Ann Oncol. 18:886–891.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Kim SY, Yoon MJ, Park YI, Kim MJ, Nam BH
and Park SR: Nomograms predicting survival of patients with
unresectable or metastatic gastric cancer who receive combination
cytotoxic chemotherapy as first-line treatment. Gastric Cancer.
21:453–463. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Takahari D, Boku N, Mizusawa J, Takashima
A, Yamada Y, Yoshino T, Yamazaki K, Koizumi W, Fukase K, Yamaguchi
K, et al: Determination of prognostic factors in Japanese patients
with advanced gastric cancer using the data from a randomized
controlled trial, Japan clinical oncology group 9912. Oncologist.
19:358–366. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Takahari D, Mizusawa J, Koizumi W, Hyodo I
and Boku N: Validation of the JCOG prognostic index in advanced
gastric cancer using individual patient data from the SPIRITS and
G-SOX trials. Gastric Cancer. 20:757–763. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Ma T, Wu Z, Zhang X, Xu H, Feng Y, Zhang
C, Xie M, Yang Y, Zhang Y, Feng C and Sun G: Development and
validation of a prognostic scoring model for mortality risk
stratification in patients with recurrent or metastatic gastric
carcinoma. BMC Cancer. 21:13262021. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Boku N, Yamamoto S, Fukuda H, Shirao K,
Doi T, Sawaki A, Koizumi W, Saito H, Yamaguchi K, Takiuchi H, et
al: Fluorouracil versus combination of irinotecan plus cisplatin
versus S-1 in metastatic gastric cancer: A randomised phase 3
study. Lancet Oncol. 10:1063–1069. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Namikawa T, Ishida N, Tsuda S, Fujisawa K,
Munekage E, Iwabu J, Munekage M, Uemura S, Tsujii S, Tamura T, et
al: Prognostic significance of serum alkaline phosphatase and
lactate dehydrogenase levels in patients with unresectable advanced
gastric cancer. Gastric Cancer. 22:684–691. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Murakami Y, Saito H, Shimizu S, Kono Y,
Shishido Y, Miyatani K, Matsunaga T, Fukumoto Y and Fujiwara Y:
Neutrophil-to-lymphocyte ratio as a prognostic indicator in
patients with unresectable gastric cancer. Anticancer Res.
39:2583–2589. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Templeton AJ, McNamara MG, Šeruga B,
Vera-Badillo FE, Aneja P, Ocaña A, Leibowitz-Amit R, Sonpavde G,
Knox JJ, Tran B, et al: Prognostic role of neutrophil-to-lymphocyte
ratio in solid tumors: A systematic review and meta-analysis. J
Natl Cancer Inst. 106:dju1242014. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Iwai N, Okuda T, Sakagami J, Harada T,
Ohara T, Taniguchi M, Sakai H, Oka K, Hara T, Tsuji T, et al:
Neutrophil to lymphocyte ratio predicts prognosis in unresectable
pancreatic cancer. Sci Rep. 10:187582020. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Shimura T, Toden S, Kandimalla R, Toiyama
Y, Okugawa Y, Kanda M, Baba H, Kodera Y, Kusunoki M and Goel A:
Genomewide expression profiling identifies a novel miRNA-based
signature for the detection of peritoneal metastasis in patients
with gastric cancer. Ann Surg. 274:e425–e434. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Emoto S, Ishigami H, Yamashita H,
Yamaguchi H, Kaisaki S and Kitayama J: Clinical significance of
CA125 and CA72-4 in gastric cancer with peritoneal dissemination.
Gastric Cancer. 15:154–161. 2012. View Article : Google Scholar : PubMed/NCBI
|