Introduction
Papillary tumor of the pineal region (PTPR) was
originally described as a distinct clinicopathological entity by
Jouvet et al in 2003 (1). In
2007, PTPR was included in the World Health Organization
classification of central nervous system tumors (2). PTPR does not arise from the pineal
gland itself, but originates from specialized cytokeratin-positive
and nestin-positive ependymal cells that are derived from the
subcommissural organ (3–5). Tumors of the pineal region are rare
lesions, accounting for only 1% of all intracranial tumors
(6). PTPR have morphological
features in common with a number of other papillary-like tumors
that occur in the pineal region, including pineal parenchymal
neoplasms, choroid plexus papilloma, papillary ependymoma,
metastatic papillary carcinomas, papillary meningioma and germ cell
tumors (5,7), which complicates the clinical diagnosis
of PTPR. Clinical presentation most often includes headache and
obstructive hydrocephalus. Microscopic evaluation often
demonstrates a lesion with papillary areas lined by epithelioid
tumors with eosinophilic cytoplasm, and numerous cells exhibiting
clear or vacuolated cytoplasm. Perivascular and true rosettes may
be identified (8). The natural
history and optimal treatment of PTPR remain controversial
(9) and Kaplan-Meier analysis
provided a 5 year survival estimate of 73% (10). The present study reports the case of
a 10-year-old patient that underwent magnetic resonance imaging
(MRI) and surgical resection of tumors of the pineal region. The
final diagnosis of PTPR was based on the morphological features of
the tumor cells and the results of immunohistochemical staining. A
written informed consent was obtained from the patient's
family.
Case report
A 10-year-old girl presented with one-year history
of right eye strabismus accompanied by diplopia, with no apparent
cause. The patient was treated with traditional Chinese medicine in
a local hospital and the diplopia symptoms were alleviated, while
the strabismus symptoms persisted. One month prior to presentation,
the patient suffered from an irregular intermittent headache,
particularly in the lateral and top areas of the forehead. During
this period, the patient additionally experienced intermittent
nausea and vomiting. For further evaluation, the patient was
admitted to the Affiliated Hospital of Qingdao University (Qingdao,
China) in March 2014. The results of a physical examination
conducted at the point of patient admission to the hospital were
unremarkable with the exception of the right eye strabismus.
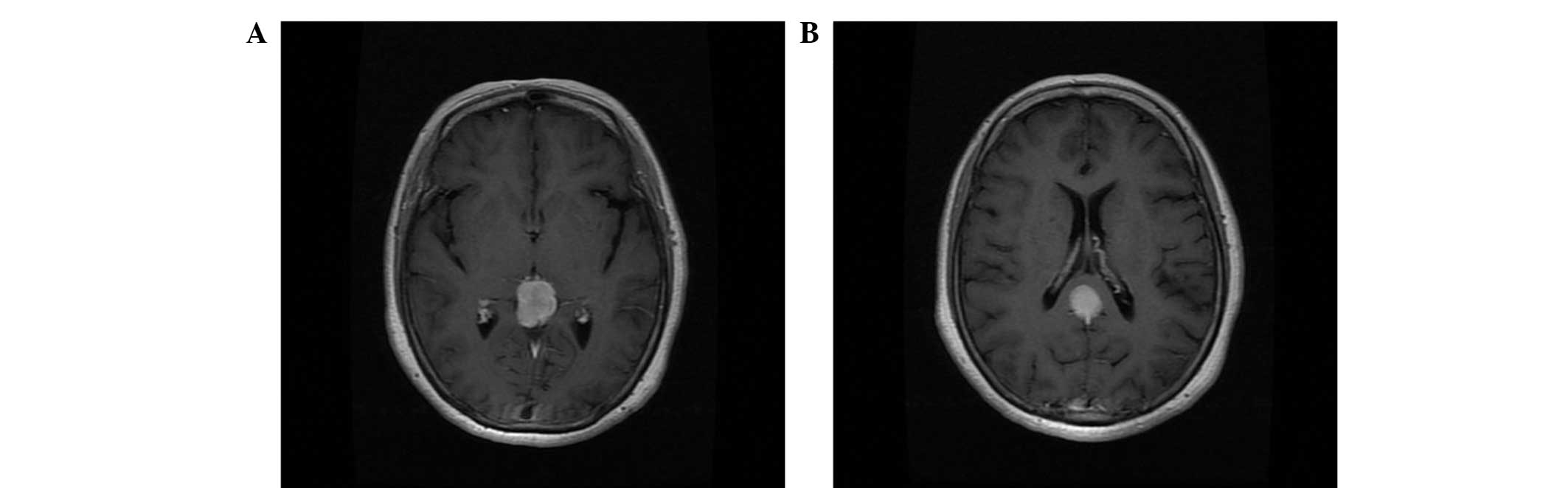
Further MRI scans demonstrated a heterogeneously-enhanced and
well-defined space-occupying lesion with limited cystic components
in the pineal region (Fig. 1). The
patient was diagnosed with hydrocephalus and abnormal cerebral
aqueduct, which was considered to be a tumor.
The tumor was removed via a suboccipital
transtentorial approach (11).
During surgery, the tumor appeared grayish, soft,
well-circumscribed and markedly vascular, exhibiting adhesion to
the deep venous system and strong adhesion to the corpora
quadrigemina. The majority of the tumor was succesfully removed,
and the patient underwent an endoscopic third ventriculostomy for
hydrocephalus management.
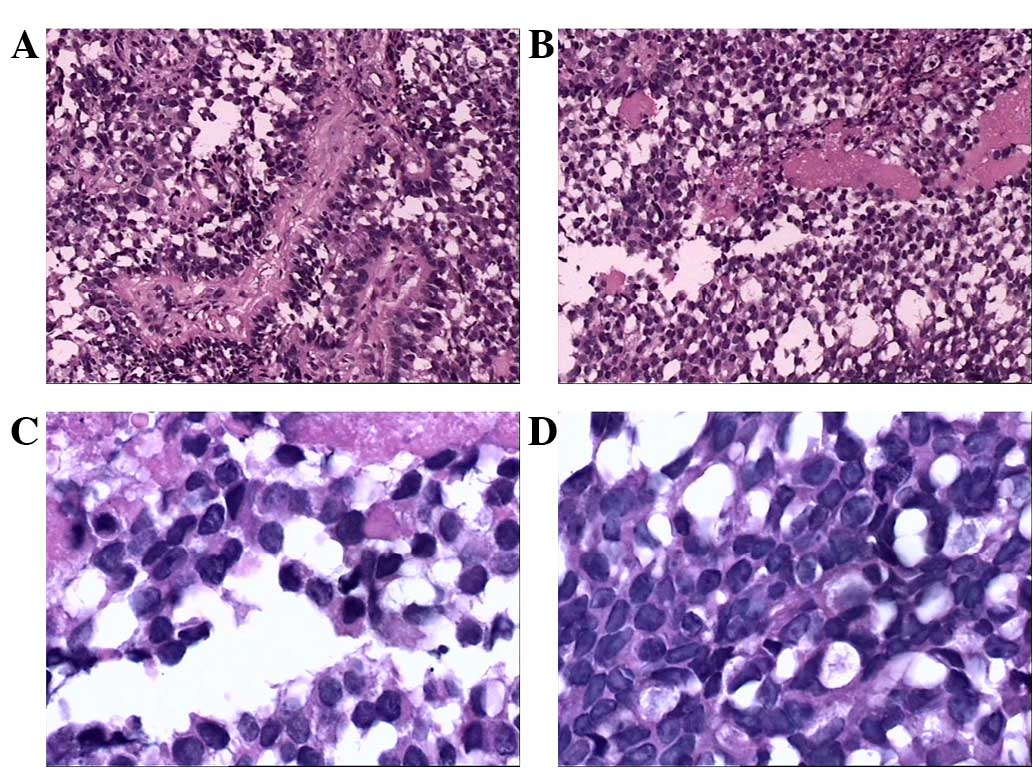
Microscopic examination revealed that parts of the
tumor exhibited papillary structures and a palisade arrangement
surrounding the vascular pseudostratified columnar epithelium was
observed. Examination of hematoxylin and eosin-stained sections
showed that the cells demonstrated papillary growth patterns. The
cytoplasm was hyperchromatic and the nuclei were slightly irregular
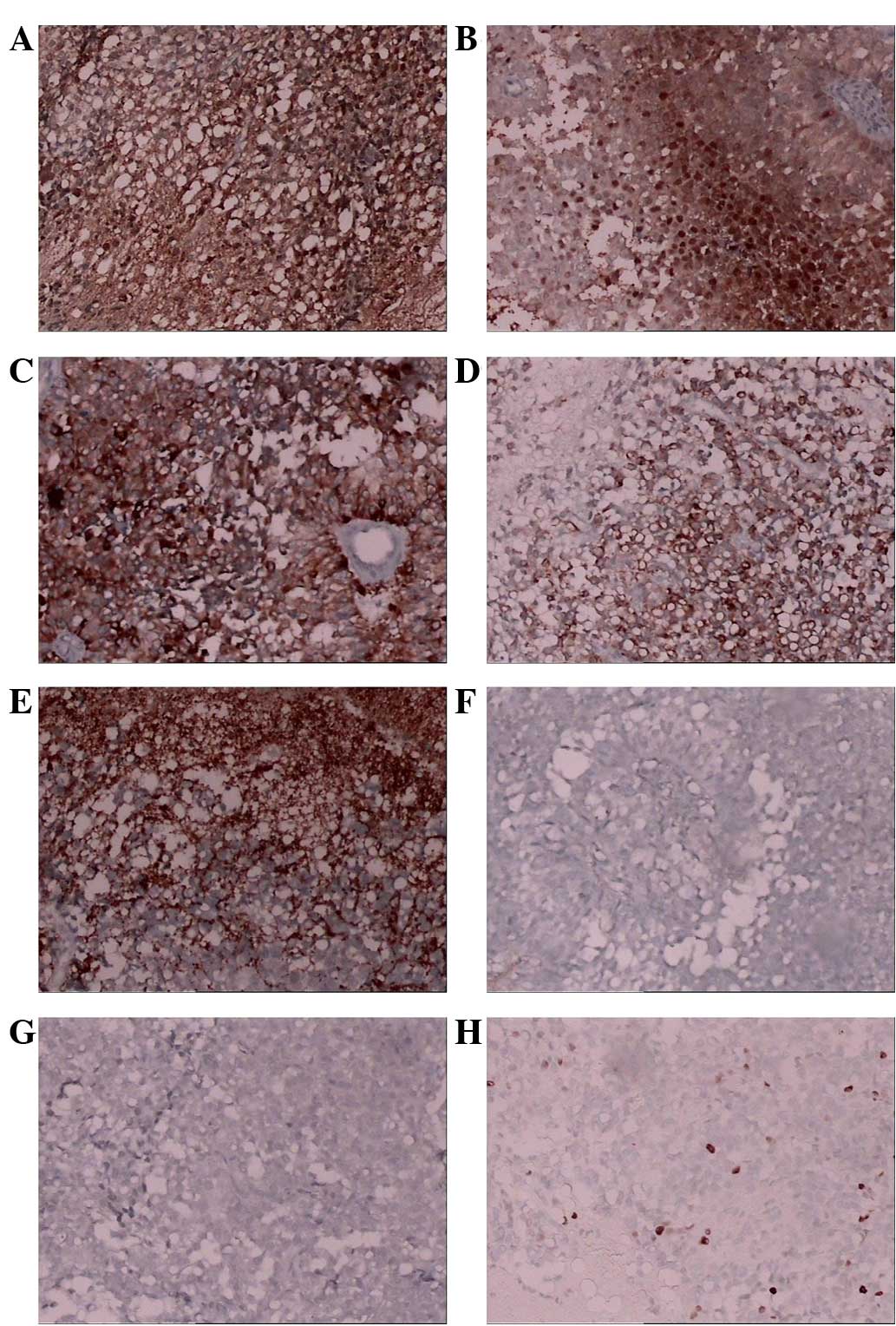
(Fig. 2). In addition,
immunohistochemical staining revealed marked immunoreactivity for
S100-protein, neuronal specific enolase, CAM5.2 and cytokeratin
8/18, while the tumor was focally immunoreactive for synaptophysin;
however, the tumor was found to be negative for glial fibrillary
acidic protein (GFAP) and epithelial membrane antigen. The Ki67
proliferative index at this initial resection was ~5% (Fig. 3). On the basis of these features, a
diagnosis of PTPR was rendered. Postoperatively, the patient
continues to do well, and no recurrent tumor was found at the
15-month follow-up examination.
Discussion
The term ‘PTPR’ is based on the histopathological
description of a tumor characterized by a papillary pattern,
rosettes and pseudorosettes (11).
Other tumors of the pineal region manifested by papillary features
include pineal parenchymal neoplasms, choroid plexus papilloma,
papillary ependymoma, metastatic papillary carcinomas, papillary
meningioma and germ cell tumors. However, pineal parenchymal
tumors, meningiomas and germ cell tumors rarely display papillary
features (12). The
immunohistochemical characteristics of PTPR include variable
immunoreactivity for cytokeratin and S-100 protein, and complete
absence of immunoreactivity for GFAP; therefore, GFAP staining aid
in distinguishing this neoplasm from an ependymoma (13,14).
Choroid plexus papilloma rarely occurred in the posterior third
ventricle. Therefore, in the present study, ultrastructural and
immunohistochemical analyses were used to distinguish this type of
papillary tumor from other papillary-like tumors that occur in the
region, and a final histological diagnosis of PTPR was
confirmed.
PTPR is an uncommon type of neoplasm and, to the
best of our knowledge, only 93 cases have been reported thus far
(14–25). Table I
summarizes 93 cases of patients with PTPR (14–25),
including 74 cases described by Poulgrain et al in 2011
(15) and 19 cases reported after
2011 (8–25). The 93 previously reported cases
include a wide range of ages. The youngest patient was a
15-month-old boy (16) and the
oldest was a 67-year-old female (15). In addition, 7 cases have been
reported in children younger than 16 years (Table II). The present study reported a
case of PTPR in a 10-year-old girl, with the proportion of children
being 7.53%. Notably, the incidence rates of PTPR in elderly
patients are low and, to the best of our knowledge, only 2 cases
have been reported in patients older than 65 years (15). By contrast, PTPR is more common among
individuals aged ~30 years (7).
Almost no difference was detected in PTPR prevalence between males
and females in the cases described (47 males vs. 46 females).
Tumors ranged between 5 and 49 mm in size. The recurrence rate was
high (67.39%) and Kaplan-Meier analysis provided a 5-year survival
estimate of 73% (10). In the
present study we report a rare case of PTPR in a 10- year old girl
who underwent a total tumour resection with no recurrence at the
15-month follow-up examination.
 | Table I.Reports of patients with papillary
tumor of the pineal region. |
Table I.
Reports of patients with papillary
tumor of the pineal region.
| Year (Ref) | Cases (n) | Age
(years)a/gender | Tumor size (mm) | Clinical
symptoms | MRI features | Surgery type | Adjuvant therapy | Follow-up
(months) | Recurrence/time
post-surgery |
|---|
| 2011 (12) | 74 | 11–67 (M, 35; F,
39) | 20–45 | H/A, N, V memory
loss | Well-circumscribed
T1-hyperintensity CE | 28 GTR 16 STR 30
NOS | 36 RT 16 CT 20 ND, 2
Nil | 0.75–218 | 12 months |
| 2011 (13) | 2 | 48/M, 36/F | 21, 18 | H/A, memory loss,
diplopia, ataxia gait | CE | 2 GTR | CT, ND | 14 18 | No |
| 2011 (14) | 1 | 15 months/M | 10 | Gait disturbance |
Well-circumscribed | ND | CT | ND | ND |
| 2011 (15) | 1 | 47/F | 30 | Ataxia |
Well-circumscribed | GTR | ND | 36 | ND |
| 2011 (16) | 3 | 30/F, 28/F, 32/M | ND | H/A, V, visual
disturbances |
Well-circumscribed | NOS | NOS | 18 | 1 case/18 months |
| 2012 (17) | 1 | 3/F | 35 | H/A, N, gait
instability | Inhomogeneous CE | GTR | CT | 36 | Yes/36 months |
| 2012 (18) | 1 | 22/M | ND | Diplopia | NOS | STR | ND | 24 | Yes/24 months |
| 2012 (19) | 2 | 48/M, 35/M | 34 | Mechanical falls,
blurry vision | Well-circumscribed
heterogeneously enhanced cystic | ND | ND | ND | ND |
| 2012 (15) | 1 | 47/M | 30 | Ataxia |
Well-circumscribed | NOS | CT | 48 | Yes/36 months |
| 2012 (20) | 1 | 23/M | ND | H/A, left facial
numbness |
T1-hyperintensity | ND | CT | 25 | No |
| 2012 (21) | 1 | 32/M | 10 | H/A, visual
disturbances | CE |
| ND | ND | ND |
| 2013 (17) | 1 | 31/M | 10 | H/A, confusion | 3 masses with
edema | ND | ND | 84 | Yes/12 months |
| 2014 (22) | 2 | 37/M, 45/F | 49, 22 | H/A, hypoacusis
tinnitus, visual loss, imbalance urinary incontinence, ataxia | CE | 2 NOS | CT, ND | 108, 17 | No |
| 2014 (11) | 1 | 23/F | ND | ND | ND | GTR | ND | 9 | Yes/3 months |
| 2015 (23) | 1 | 17/M | ND | H/A |
T1-hyperintensity | NOS | ND | 6 | No |
| Table II.Clinicopathological characteristics of
patients with papillary tumor of the pineal region in the reviewed
literature. |
Table II.
Clinicopathological characteristics of
patients with papillary tumor of the pineal region in the reviewed
literature.
| Characteristic | Total cases, n | Percentage of the
cases, % |
|---|
| Age, years |
|
|
|
≤16 | 7 |
7.53 |
|
16–65 | 84 | 90.32 |
|
≥65 | 2 |
2.15 |
| Gender |
|
|
|
Female | 46 | 49.46 |
|
Male | 47 | 50.54 |
| Size, mm |
|
|
|
≤10 | 3 | 10.71 |
|
>10 | 25 | 89.29 |
| Recurrence |
|
|
|
Yes | 31 | 67.39 |
| No | 15 | 32.61 |
Clinical data concerning PTPR is limited and its
pathogenesis is unknown. PTPR is frequently misdiagnosed as
ependymoma or choroids plexus papilloma. However, the diagnostic
criteria of certain postulated papillary-like tumors have been
revised, and a more complete understanding of this tumor may be
obtained. The present study reported a case of PTPR in a 10
year-old girl who suffered from an irregular intermittent headache,
particularly in the lateral and top areas of the forehead. The
patient were treated with Chinese medicine which alleviated the
diplopia symptoms. Similarly to previous reports they underwent
magnetic resonance imaging and surgical tumor resection, and
continues to have a positive postoperative outcome. These results
along with the data from previous studies indicate that total tumor
resection is the optimal treatment guideline.
Acknowledgements
This study was supported by a National Nature
Science Foundation grant (no. 81471958).
References
|
1
|
Jouvet A, Fauchon F, Liberski P,
Saint-Pierre G, Didier-Bazes M, Heitzmann A, Delisle MB, Biassette
HA, Vincent S, Mikol J, et al: Papillary tumor of the pineal
region. Am J Surg Pathol. 27:505–512. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Louis DN, Ohgaki H, Wiestler OD, Cavenee
WK, Burger PC, Jouvet A, Scheithauer BW and Kleihues P: The 2007
WHO classification of tumours of the central nervous system. Acta
Neuropatholo. 114:97–109. 2007. View Article : Google Scholar
|
|
3
|
Li J, Recinos PF, Orr BA, Burger PC, Jallo
GI and Recinos VR: Papillary tumor of the pineal region in a
15-month-old boy. J Neurosurg Pediatr. 7:534–538. 2011.PubMed/NCBI
|
|
4
|
Montange MF, Vasiljevic A, Champier J and
Jouvet A: Papillary tumor of the pineal region: Histopathological
characterization and review of the literature. Neurochirurgie.
61:138–142. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Vandergriff C, Opatowsky M, O'Rourke B and
Layton K: Papillary tumor of the pineal region. Proc (Bayl Univ Med
Cent). 25:78–79. 2012.PubMed/NCBI
|
|
6
|
Bruce JN and Stein B: Pineal tumors.
Neurosurg Clin N Am. 1:123–138. 1990.PubMed/NCBI
|
|
7
|
Kawahara I, Tokunaga Y, Yagi N, Iseki M,
Abe K and Hayashi T: Papillary tumor of the pineal region. Neurol
Med Chir (Tokyo). 47:568–571. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Rickard KA, Parker JR, Vitaz TW, Plaga AR,
Wagner S and Parker JC Jr: Papillary Tumor of the Pineal Region:
Two Case studies and a review of the literature. Ann Clin Lab Sci.
41:174–181. 2011.PubMed/NCBI
|
|
9
|
Inoue T, Kumabe T, Kanamori M, Sonoda Y,
Watanabe M and Tominaga T: Papillary tumor of the pineal region: A
case report. Brain Tumor Pathol. 25:85–90. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Boco T, Aalaei S, Musacchio M, Byrne R and
Cochran E: Papillary tumor of the pineal region. Neuropathology.
28:87–92. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Junior GV, Dellaretti M, de Carvalho GT,
Brandão RA, Mafra A and de Sousa AA: Papillary tumor of the pineal
region. Brain Tumor Patholo. 28:329–334. 2011. View Article : Google Scholar
|
|
12
|
Chang AH, Fuller GN, Debnam JM, Karis JP,
Coons SW, Ross JS and Dean BL: MR imaging of papillary tumor of the
pineal region. AJNR Am J Neuroradio. 29:187–189. 2008. View Article : Google Scholar
|
|
13
|
Kawahara I, Tokunaga Y, Yagi N, Iseki M,
Abe K and Hayashi T: Papillary tumor of the pineal region. Neurolo
Med Chir (Tokyo). 47:568–571. 2007. View Article : Google Scholar
|
|
14
|
Sun IS, Kirollos R and Santarius T: No
5-ALA fluorescence seen in a recurrent papillary tumour of the
pineal region (PTPR). Acta Neurochir (Wien). 157:215–216. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Poulgrain K, Gurgo R, Winter C, Ong B and
Lau Q: Papillary tumour of the pineal region. J Clin Neurosci.
18:1007–1017. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Li J, Recinos PF, Orr BA, Burger PC, Jallo
GI and Recinos VR: Papillary tumor of the pineal region in a
15-month-old boy. J Neurosurg Pediatr. 7:534–538. 2011.PubMed/NCBI
|
|
17
|
Santoro A, D'Elia A, Fazzolari B, Santoro
F, Antonelli M, Giangaspero F, Brogna C, Lenzi J, Frati A and
Salvati M: Four-year clinical and neuroradiological follow-up of a
papillary tumor of the pineal region. Neurol Sci. 33:931–935. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Matyja E, Grajkowska W, Nauman P and
Bonicki W: Histopathological patterns of papillary tumour of the
pineal region. Folia Neuropathol. 49:181–190. 2011.PubMed/NCBI
|
|
19
|
Abela L, Rushing EJ, Ares C, Scheer I,
Bozinov O, Boltshauser E and Grotzer MA: Pediatric papillary tumors
of the pineal region: To observe or to treat following gross total
resection? Childs Nerv Syst. 29:307–310. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Ishida A, Shibuya M, Komori T, Nobusawa S,
Niimura K, Matsuo S and Hori T: Papillary tumor of the pineal
region: A case involving isocitrate dehydrogenase (IDH) genotyping.
Brain Tumor pathol. 30:45–49. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Magalhêes J, Rostad S, Foltz G, Pytel P
and Rodriguez FJ: Cellular pleomorphism in papillary tumors of the
pineal region. Brain Tumor Pathol. 30:93–98. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Patel SK, Tomei KL, Christiano LD, Baisre
A and Liu JK: Complete regression of papillary tumor of the pineal
region after radiation therapy: Case report and review of the
literature. J Neurooncol. 107:427–434. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Vandergriff C, Opatowsky M, O'Rourke B and
Layton K: Papillary tumor of the pineal region. Proc (Bayl Univ Med
Cent). 25:78–79. 2012.PubMed/NCBI
|
|
24
|
Koziarski A, Grala B and Skrobowska E:
Papillary tumor of the pineal region. Report of two cases and
literature review. Neurol Neurochir Pol. 48:356–362.
2014.PubMed/NCBI
|
|
25
|
Rosa Junior M, da Rocha AJ, Zanon da Silva
A and Rosemberg S: Papillary tumor of the pineal region: MR Signal
intensity correlated to histopathology. Case Rep Neurol Med.
2015:3150952015.PubMed/NCBI
|