Introduction
Osteosarcoma is a type of malignant bone tumor in
which the neoplastic cells produce osteoid or bone (1). Osteosarcomas of the jaw are rare and
represent only 2–10% of all osteosarcomas. Osteosarcoma of the head
and neck region is the most common primary malignant bone tumor,
representing 23% of all head and neck malignancies (2). Osteosarcoma arises more frequently in
the maxilla compared with the mandible (3). Unlike the hallmark clinical
presentation of pain in lesions of the long bones, the most
characteristic symptom of jaw osteosarcoma is swelling. Similar
with osteosarcoma of long bones, the dominant histological variant
of osteosarcoma is the osteoblastic type, followed by the
chondroblastic and fibroblastic types (4). However, the pathologist may encounter a
potential diagnostic pitfall when an osteosarcoma of the jaw
resembles a cemento-osseous lesion. We herein present a case of
maxillary osteosarcoma mimicking the histological and radiographic
characteristics of cemento-osseous lesions.
Case report
A 53-year-old male patient presented in May, 2014
with gradual swelling of the left side of the face over a period of
4 years. The patient's medical history was non-contributory. The
physical examination revealed an uncircumscribed swelling of the
left maxilla, with normal color of the overlying skin. A panoramic
radiograph revealed an ill-defined radiopaque mass at the apices of
the roots of the left maxillary bone, from the incisor to the
second bicuspid (Fig. 1). The mass
was unilateral and closely associated with the teeth roots;
however, there was no root resorption in the involved teeth.
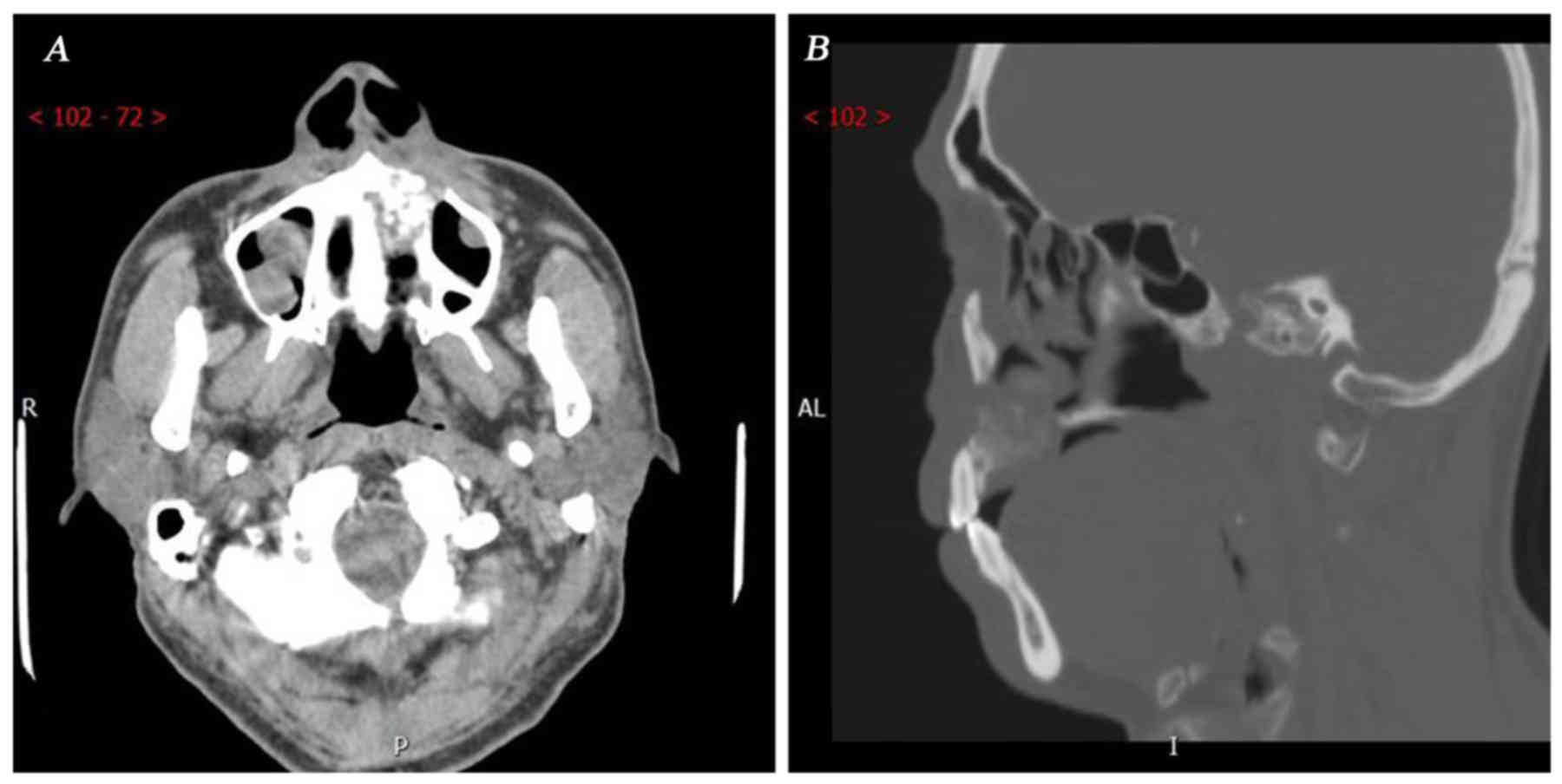
Further computed tomography examination revealed that the size of
the mass was 2.3×2×1.7 cm. No periosteal reaction was observed, and
no soft tissue extension component beyond the area of the
cancellous and/or cortical bone destruction was identified
radiographically. The lesion involved the left wall of the incisive
canal and the left hard palate, resulting in a discontinuous labial
and palatal alveolar bone plate (Fig.
2A). The corresponding nasal bottom and left wall of the
maxillary sinus were eroded (Fig.
2B). Given its association with the teeth root and the diffuse
borders, the most likely clinical diagnosis was a malignant tumor
originating from cementum. The tumor was treated by radical
resection of the left maxillary bone.
The specimens were fixed in 10% buffered formalin,
dehydrated through graded concentrations of ethanol and embedded in
paraffin wax. The paraffin block was then cut in 4-mm sections that
were stained with haematoxylin and eosin (H&E).
Grossly, the tumor involved alveolar bone as well as
bone from the body of the maxilla, from the first incisor to the
proximal side of the first molar (Fig.
3). All the roots of the involved teeth were partially embedded
in the tumor. The tumor appeared as pale, without clear borders
from the surrounding bone tissue. The sectional area of the mass
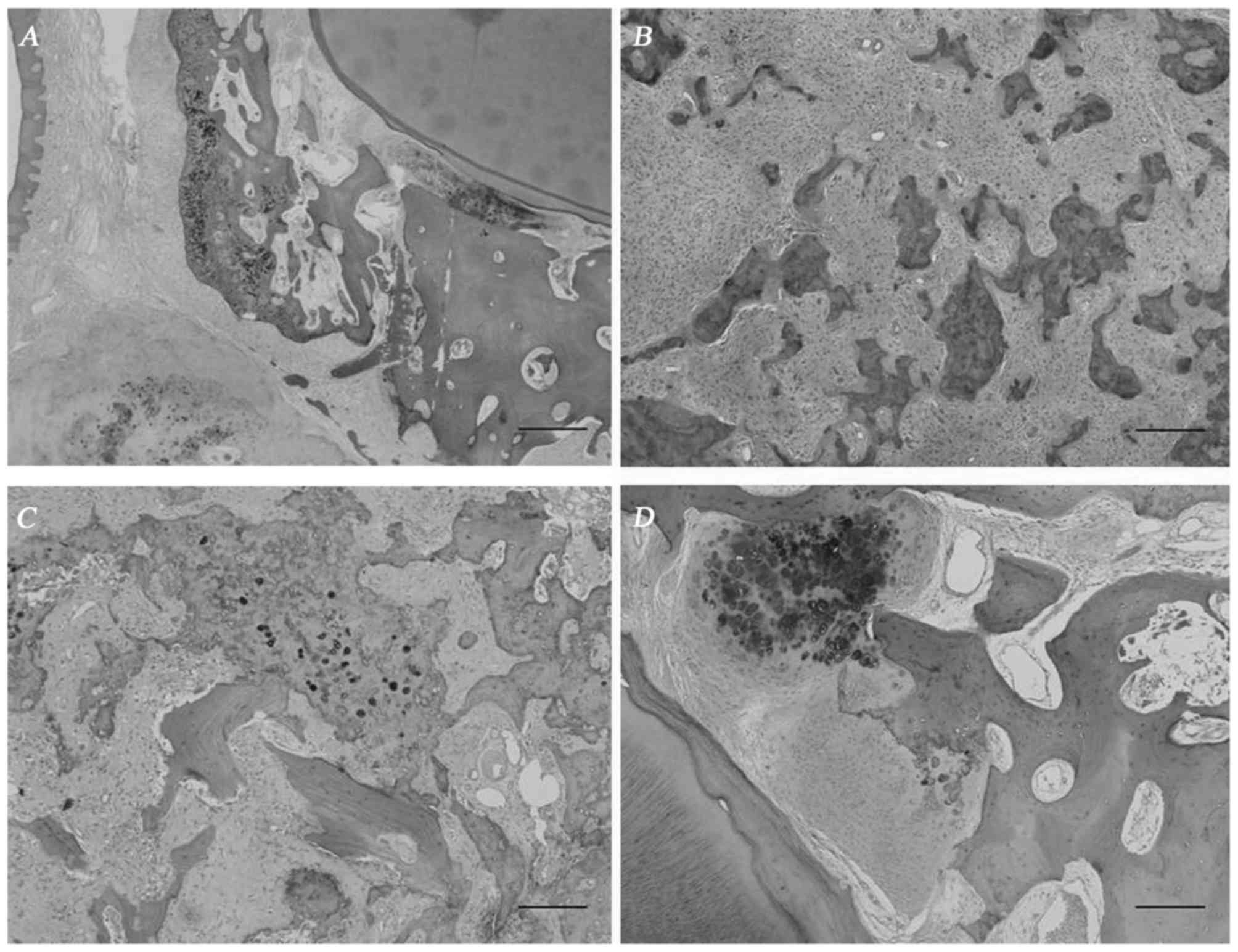
was 3.4×3 cm. Microscopically, the mass displayed a different
appearance in the alveolar bone and in the body of the jaw. In the
alveolar bone part, the tumor infiltrated the periodontal ligament
and alveolar bone proper (Fig. 4A).
Extensive cementicle-like structure and deposits of hypercellular
cartilage were observed in the alveolar bone (Fig. 4B). However, this cementum-like
material was intimately associated with the pleomorphic and
hyperchromatic spindle cell component, and it infiltrated the
trabeculae of the medullary bone (Fig.
4C), suggesting a malignant tumor. Interestingly, a continuous
transition from the trabecular alveolar bone to the tumor was
observed at the bony side of the periodontal ligament, strongly
supporting the hypothesis that the tumor originated from bone, not
from the periodontal ligament, and suggesting that the tumor would
differentiate towards osteoid and not towards cementum-like
material.
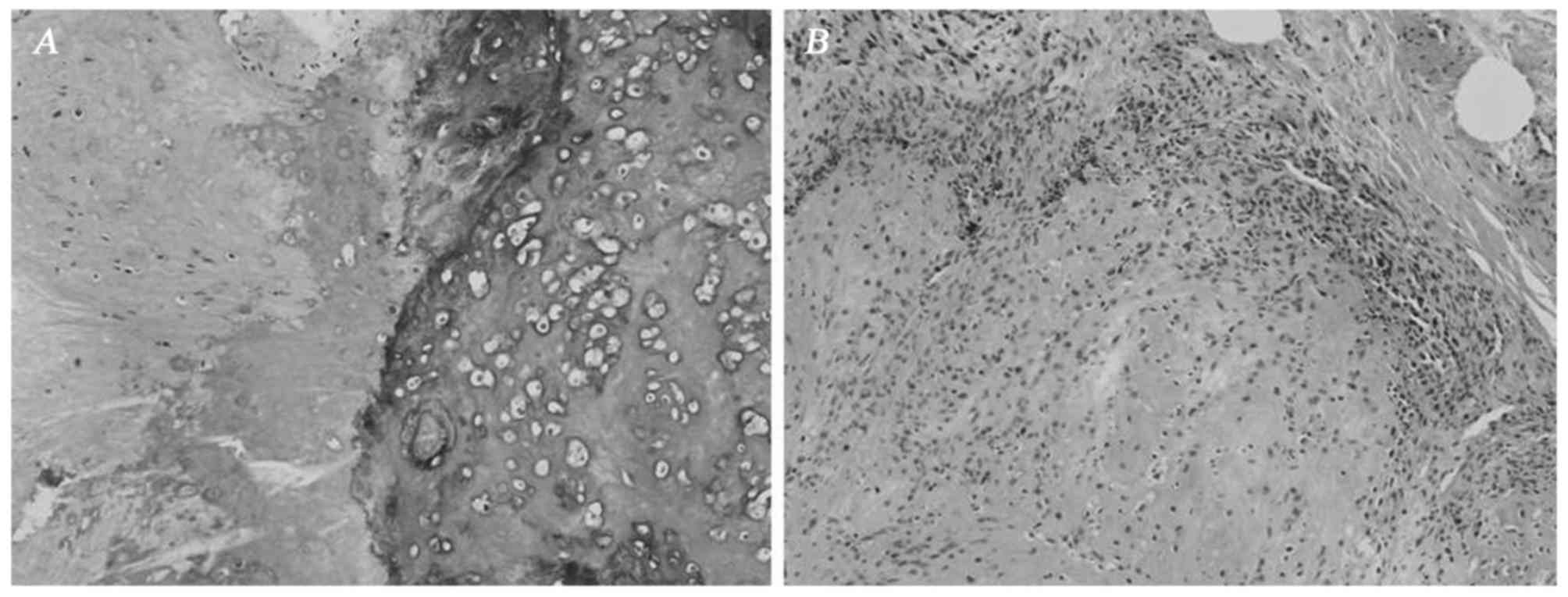
In the bone of the maxilla, the mass exhibited the
morphological characteristics of a typical chondroblastic
osteosarcoma. The tumor contained a relatively equal distribution
of abnormal osteoid and chondroid, intimately associated with
anaplastic tumor cells (Fig. 5A).
Islands of osteoid were observed within the cartilage. The tumor
bone exhibited a woven or basket weave pattern and was strongly
hematoxylinophilic, unlike the uniform lamellar pattern of normal
bone. The cartilage displayed malignant-appearing cells in lacunae,
and there was crowding at the periphery of the lobule, where
spindle cells were arranged in sheets (Fig. 5B).
Discussion
Osteosarcoma is characterized by the osteoid
production by tumor cells. Osteosarcoma of the jaw is associated
with certain specific characteristics, such as a higher prevalence
in the maxilla and male predominance. Wang et al reported
that all maxillary de novo osteosarcomas arose from the
alveolar ridge (5). The mass in the
present case involved both the alveolar ridge and the body of the
maxilla, possibly due to long-term growth leading to extension of
the mass from the alveolar ridge to the body.
The differential diagnosis between lesions with hard
tissue formation may be problematic in the oral area. These lesions
are associated with the formation of bone, cartilage or cementum.
Among these, osteosarcoma may arise de novo, may be
synchronous multicentric (6),
metastatic (7), or appear in benign
precursor lesions, which may include cemento-osseous dysplasia
(8) or ossifying fibroma (9). Cemento-osseous lesions are lesions of
the jaw closely associated with the apices of the teeth that
contain amorphous spherical calcifications resembling an aberrant
form of cementum.
Specifically for this case, the differential
diagnosis among primary osteosarcoma, concurrent cemento-osseous
dysplasia and secondary malignant tumor in a background of
cemento-osseous dysplasia or ossifying fibroma, may be difficult
radiographically as well as histopathologically. Generally, the
suspected clinical diagnosis was a cementum-originating tumor due
to its association with the roots of the teeth and absence of
periosteal reaction. The pathological appearance in the alveolar
bone was confusing due to the presence of a cementicle-like
structure. However, the typical manifestations in the body of the
maxilla provided strong evidence for the diagnosis of primary
chondroblastic osteosarcoma.
The mechanisms underlying the formation of bone,
cartilage, or cementum in the oral area are helpful for
understanding the nature of the lesions involving hard tissue
formation, and may provide clues for differential diagnosis. Cells
forming bone in the jaw may be divided into three types:
Osteoblasts lying on the bone surface, osteogenic fibroblasts in
the periodontal ligament and periosteum, and non-specific
fibroblasts stimulated to differentiate into osteogenic cells after
degeneration (10). The first two
cell types are associated with the origin of jaw osteosarcoma,
whereas the osteogenic cells in the periodontal ligament produce
cementum (11). Therefore, the tumor
cells responsible for hard tissue formation in osteosarcoma,
cemento-osseous dysplasia or ossifying fibroma, may share a common
origin. This may explain the presence of the cementicle-like
structure in this osteosarcoma. However, cementum is a bone-like
tissue that covers the root of the tooth. Cementocytes are similar
to osteocytes, but their cell processes tend to be orientated in
one direction, namely towards the periodontal ligament, rather than
equally around the cell body, as in osteocytes. Therefore, what was
referred to as a cementicle-like structure in this case was in fact
abnormal osteoid structure of osteosarcoma. Osteoid displays a
woven or mat-like appearance, unlike the more orderly longitudinal
fiber array found in collagen.
References
|
1
|
Sato K and Unni KK: Malignant tumors of
bone and cartilagePathology and Genetics of Head and Neck Tumors:
World Health Organization Classification of Tumors. Barnes L,
Eveson JW, Reichart P and Sidransky D: IARC Press; Lyon: pp. 7–52.
2005
|
|
2
|
Nthumba PM: Osteosarcoma of the jaws: A
review of literature and a case report on synchronous multicentric
osteosarcomas. World J Surg Oncol. 10:2402012. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Forteza G, Colmenero B and López-Barea F:
Osteogenic sarcoma of maxilla and mandible. Oral Surg Oral Med Oral
Pathol. 62:179–184. 1986. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Paparella ML, Olvi LG, Brandizzi D,
Keszler A, Santini-Araujo E and Cabrini RL: Osteosarcoma of the
jaw: An analysis of a series of 74 cases. Histopathology.
63:551–557. 2013.PubMed/NCBI
|
|
5
|
Wang S, Shi H and Yu Q: Osteosarcoma of
the jaws: Demographic and CT imaging features. Dentomaxillofac
Radiol. 41:37–42. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Jia S and Li B: Osteosarcoma of the Jaws:
Case report on synchronous multicentric osteosarcomas. J Clin Diagn
Res. 8:ZD01–ZD03. 2014.PubMed/NCBI
|
|
7
|
Carnelio S, Pai K, Rao N, Solomon M and
Ahasan A: Metastatic osteosarcoma to the maxilla: A case report and
a review of the literature. Quintessence Int. 33:397–399.
2002.PubMed/NCBI
|
|
8
|
Olusanya AA, Adeyemi BF and Adisa AO:
Concurrent cemento-osseous dysplasia and osteogenic sarcoma: Report
of two cases. Case Rep Med. 2012:1805612012.PubMed/NCBI
|
|
9
|
Koury ME, Regezi JA, Perrott DH and Kaban
LB: ‘Atypical’ fibro-osseous lesions: Diagnostic challenges and
treatment concepts. Int J Oral Maxillofac Surg. 24:162–169. 1995.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Matsuzaka K, Shimono M, Uchiyama T, Noma H
and Inoue T: Lesions related to the formation of bone, cartilage or
cementum arising in the oral area: A statistical study and review
of the literature. Bull Tokyo Dent Coll. 43:173–180. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Roguljic H, Matthews BG, Yang W, Cvija H,
Mina M and Kalajzic I: In vivo identification of periodontal
progenitor cells. J Dent Res. 92:709–715. 2013. View Article : Google Scholar : PubMed/NCBI
|