|
1
|
Committee on the Treatment of Cardiac
Arrest; Current Status and Future Directions; Board on Health
Sciences Policy and Institute of Medicine: Strategies to Improve
Cardiac Arrest Survival: A Time to Act. Graham R, McCoy MA and
Schultz AM (eds). National Academies Press, Washington, DC,
2015.
|
|
2
|
Nichol G and Soar J: Regional cardiac
resuscitation systems of care. Curr Opin Crit Care. 16:223–230.
2010.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Böttiger BW and Van Aken HK: Saving
100,000 lives each year in Europe. Best Pract Res Clin
Anaesthesiol. 27:291–292. 2013.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Goyal A, Sciammarella JC, Cusick AS and
Patel PH: Cardiopul-monary resuscitation. In: StatPearls
[Internet]. StatPearls Publishing, Treasure Island, FL, 2024.
|
|
5
|
Şan İ, Bekgöz B, Ergin M and Usul E:
Manual cardiopulmonary resuscitation versus mechanical
cardiopulmonary resuscitation: Which one is more effective during
ambulance transport? Turk J Emerg Med. 21:69–74. 2021.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Couper K, Smyth M and Perkins GD:
Mechanical devices for chest compression: To use or not to use?
Curr Opin Crit Care. 21:188–194. 2013.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Poole K, Couper K, Smyth MA, Yeung J and
Perkins GD: Mechanical CPR: Who? When? How? Crit Care.
22(140)2018.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Chiang CY, Lim KC, Lai PC, Tsai TY, Huang
YT and Tsai MJ: Comparison between prehospital mechanical
cardiopulmonary resuscitation (CPR) devices and manual CPR for
out-of-hospital cardiac arrest: A systematic review, meta-analysis,
and trial sequential analysis. J Clin Med. 11(1448)2022.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Bonnes JL, Brouwer MA, Navarese EP,
Verhaert DVM, Verheugt FWA, Smeets JLRM and de Boer MJ: Manual
cardiopulmonary resuscitation versus CPR including a mechanical
chest compression device in out-of-hospital cardiac arrest: A
comprehensive meta-analysis from randomized and observational
studies. Ann Emerg Med. 67:349–360.e3. 2016.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Tang L, Gu WJ and Wang F: Mechanical
versus manual chest compressions for out-of-hospital cardiac
arrest: A meta-analysis of randomized controlled trials. Sci Rep.
5(15635)2015.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Zhu N, Chen Q, Jiang Z, Liao F, Kou B,
Tang H and Zhou M: A meta-analysis of the resuscitative effects of
mechanical and manual chest compression in out-of-hospital cardiac
arrest patients. Crit Care. 23(100)2019.PubMed/NCBI View Article : Google Scholar
|
|
12
|
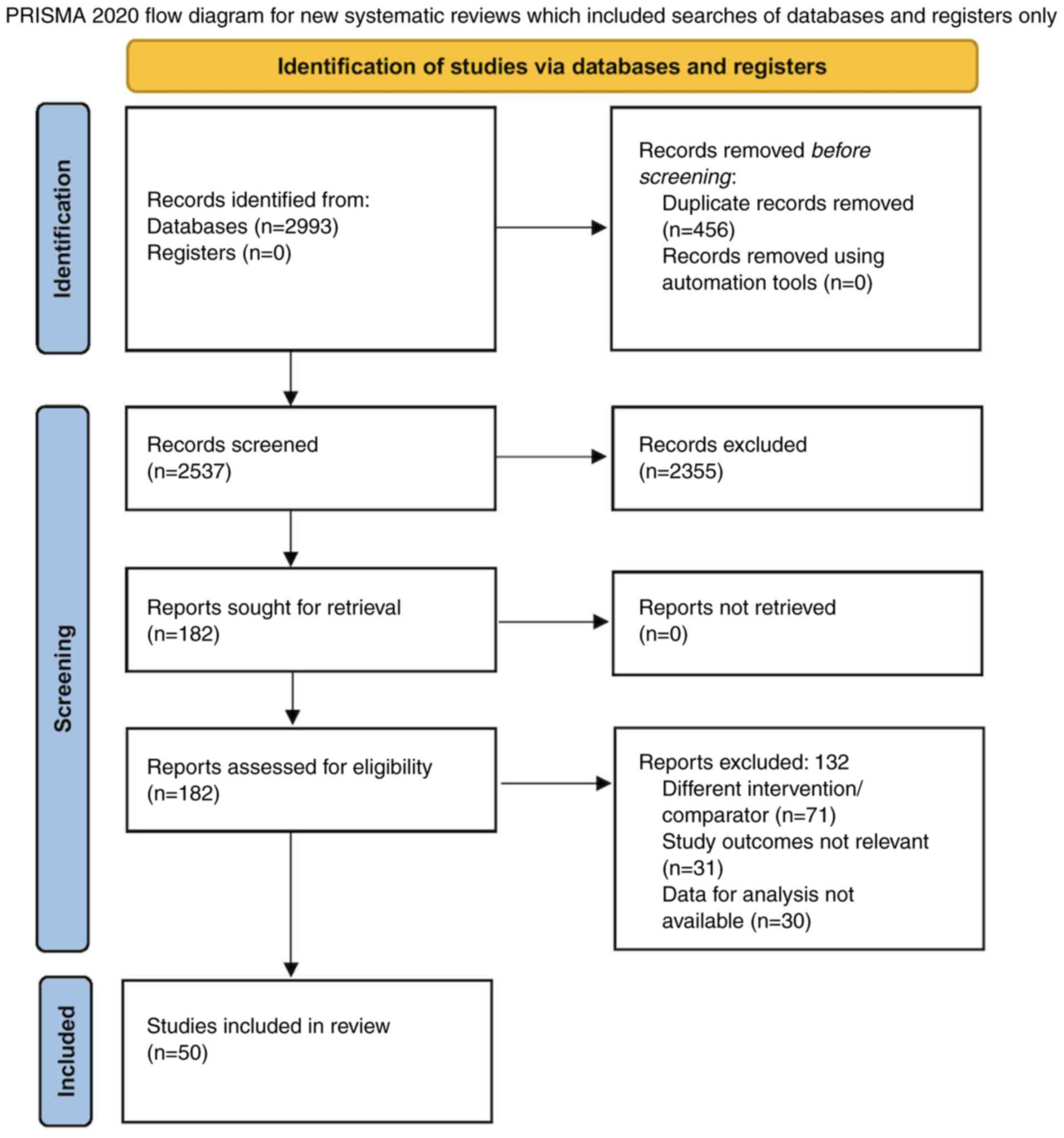
Page MJ, McKenzie JE, Bossuyt PM, Boutron
I, Hoffmann TC, Mulrow CD, Shamseer L, Tetzlaff JM, Akl EA, Brennan
SE, et al: The PRISMA 2020 statement: An updated guideline for
reporting systematic reviews. Int J Surg. 88(105906)2021.PubMed/NCBI View
Article : Google Scholar
|
|
13
|
Sterne JA, Savović J, Page MJ, Elbers RG,
Blencowe NS, Boutron I, Cates CJ, Cheng HY, Corbett MS, Eldridge
SM, et al: RoB 2: A revised tool for assessing risk of bias in
randomised trials. BMJ. 366(l4898)2019.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Sterne JA, Hernán MA, Reeves BC, Savović
J, Berkman ND, Viswanathan M, Henry D, Altman DG, Ansari MT,
Boutron I, et al: ROBINS-I: A tool for assessing risk of bias in
non-randomised studies of interventions. BMJ.
355(i4919)2016.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Cumpston M, Li T, Page MJ, Chandler J,
Welch VA, Higgins JP and Thomas J: Updated guidance for trusted
systematic reviews: A new edition of the cochrane handbook for
systematic reviews of interventions. Cochrane Database Syst Rev.
10(ED000142)2019.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Furuya-Kanamori L, Barendregt JJ and Doi
SAR: A new improved graphical and quantitative method for detecting
bias in meta-analysis. Int J Evid Based Healthc. 16:195–203.
2018.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Zhang Y, Coello PA, Guyatt GH, Yepes-Nuñez
JJ, Akl EA, Hazlewood G, Pardo-Hernandez H, Etxeandia-Ikobaltzeta
I, Qaseem A, Williams JW Jr, et al: GRADE guidelines: 20. Assessing
the certainty of evidence in the importance of outcomes or values
and preferences-inconsistency, imprecision, and other domains. J
Clin Epidemiol. 111:83–93. 2019.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Seewald S, Obermaier M, Lefering R, Bohn
A, Georgieff M, Muth CM, Gräsner JT, Masterson S, Scholz J and
Wnent J: Application of mechanical cardiopulmonary resuscitation
devices and their value in out-of-hospital cardiac arrest: A
retrospective analysis of the German resuscitation registry. PLoS
One. 14(e0208113)2019.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Smekal D, Johansson J, Huzevka T and
Rubertsson S: A pilot study of mechanical chest compressions with
the LUCAS™ device in cardiopulmonary resuscitation.
Resuscitation. 82:702–706. 2011.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Jennings PA, Harriss L, Bernard S, Bray J,
Walker T, Spelman T, Smith K and Cameron P: An automated CPR device
compared with standard chest compressions for out-of-hospital
resuscitation. BMC Emerg Med. 12(8)2012.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Buckler DG, Burke RV, Naim MY, MacPherson
A, Bradley RN, Abella BS and Rossano JW: CARES Surveillance Group.
Association of mechanical cardiopulmonary resuscitation device use
with cardiac arrest outcomes: A population-based study using the
CARES registry (cardiac arrest registry to enhance survival).
Circulation. 134:2131–2133. 2016.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Ujvárosy D, Sebestyén V, Pataki T, Ötvös
T, Lőrincz I, Paragh G and Szabó Z: Cardiovascular risk factors
differently affect the survival of patients undergoing manual or
mechanical resuscitation. BMC Cardiovasc Disord.
18(227)2018.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Axelsson C, Nestin J, Svensson L, Axelsson
AB and Herlitz J: Clinical consequences of the introduction of
mechanical chest compression in the EMS system for treatment of
out-of-hospital cardiac arrest-a pilot study. Resuscitation.
71:47–55. 2006.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Gao C, Chen Y, Peng H, Chen Y, Zhuang Y
and Zhou S: Clinical evaluation of the AutoPulse automated chest
compression device for out-of-hospital cardiac arrest in the
northern district of Shanghai, China. Arch Med Sci. 12:563–570.
2016.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Tantarattanapong S and Chantaramanee K:
Comparison of sustained return of spontaneous circulation rate
between manual and mechanical chest compression in adult cardiac
arrest. Open Access Emerg Med. 14:599–608. 2022.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Lin CK, Huang MC, Feng YT, Jeng WH, Chung
TC, Lau YW and Cheng KI: Effectiveness of mechanical chest
compression for out-of-hospital cardiac arrest patients in an
emergency department. J Chin Med Assoc. 78:360–363. 2015.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Dickinson ET, Verdile VP, Schneider RM and
Salluzzo RF: Effectiveness of mechanical versus manual chest
compressions in out-of-hospital cardiac arrest resuscitation: A
pilot study. Am J Emerg Med. 16:289–292. 1998.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Satterlee PA, Boland LL, Johnson PJ,
Hagstrom SG, Page DI and Lick CJ: Implementation of a mechanical
chest compression device as standard equipment in a large
metropolitan ambulance service. J Emerg Med. 45:562–569.
2013.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Axelsson C, Herrera MJ, Fredriksson M,
Lindqvist J and Herlitz J: Implementation of mechanical chest
compression in out-of-hospital cardiac arrest in an emergency
medical service system. Am J Emerg Med. 31:1196–1200.
2013.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Hock Ong ME, Fook-Chong S, Annathurai A,
Ang SH, Tiah L, Yong KL, Koh ZX, Yap S and Sultana P: Improved
neurologically intact survival with the use of an automated,
load-distributing band chest compression device for cardiac arrest
presenting to the emergency department. Crit Care.
16(R144)2012.PubMed/NCBI View
Article : Google Scholar
|
|
31
|
Steinmetz J, Barnung S, Nielsen SL, Risom
M and Rasmussen LS: Improved survival after an out-of-hospital
cardiac arrest using new guidelines. Acta Anaesthesiol Scand.
52:908–913. 2008.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Savastano S, Baldi E, Palo A, Raimondi M,
Belliato M, Compagnoni S, Buratti S, Cacciatore E, Canevari F,
Iotti G, et al: Load distributing band device for mechanical chest
compressions: An Utstein-categories based analysis of survival to
hospital discharge. Int J Cardiol. 287:81–85. 2019.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Karasek J, Ostadal P, Klein F, Rechova A,
Seiner J, Strycek M, Polasek R and Widimsky P: LUCAS II device for
cardiopulmonary resuscitation in a nonselective out-of-hospital
cardiac arrest population leads to worse 30-day survival rate than
manual chest compressions. J Emerg Med. 59:673–679. 2020.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Hallstrom A, Rea TD, Sayre MR, Christenson
J, Anton AR, Mosesso VN Jr, Van Ottingham L, Olsufka M, Pennington
S, White LJ, et al: Manual chest compression vs use of an automated
chest compression device during resuscitation following
out-of-hospital cardiac arrest: A randomized trial. JAMA.
295:2620–2628. 2006.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Wik L, Olsen JA, Persse D, Sterz F, Lozano
M Jr, Brouwer MA, Westfall M, Souders CM, Malzer R, van Grunsven
PM, et al: Manual vs integrated automatic load-distributing band
CPR with equal survival after out of hospital cardiac arrest. The
randomized CIRC trial. Resuscitation. 85:741–748. 2014.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Hayashida K, Tagami T, Fukuda T, Suzuki M,
Yonemoto N, Kondo Y, Ogasawara T, Sakurai A, Tahara Y, Nagao K, et
al: Mechanical cardiopulmonary resuscitation and hospital survival
among adult patients with nontraumatic out-of-hospital cardiac
arrest attending the emergency department: a prospective,
multicenter, observational study in Japan [SOS-KANTO (survey of
survivors after out-of-hospital cardiac arrest in Kanto Area) 2012
study]. J Am Heart Assoc. 6(e007420)2017.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Jung E, Park JH, Lee SY, Ro YS, Hong KJ,
Song KJ, Ryu HH and Shin SD: Mechanical chest compression device
for out-of-hospital cardiac arrest: A nationwide observational
study. J Emerg Med. 58:424–431. 2020.PubMed/NCBI View Article : Google Scholar
|
|
38
|
Zeiner S, Sulzgruber P, Datler P,
Keferböck M, Poppe M, Lobmeyr E, van Tulder R, Zajicek A, Buchinger
A, Polz K, et al: Mechanical chest compression does not seem to
improve outcome after out-of hospital cardiac arrest. A single
center observational trial. Resuscitation. 96:220–225.
2015.PubMed/NCBI View Article : Google Scholar
|
|
39
|
Rubertsson S, Lindgren E, Smekal D,
Östlund O, Silfverstolpe J, Lichtveld RA, Boomars R, Ahlstedt B,
Skoog G, Kastberg R, et al: Mechanical chest compressions and
simultaneous defibrillation vs conventional cardiopulmonary
resuscitation in out-of-hospital cardiac arrest: The LINC
randomized trial. JAMA. 311:53–61. 2014.PubMed/NCBI View Article : Google Scholar
|
|
40
|
Perkins GD, Lall R, Quinn T, Deakin CD,
Cooke MW, Horton J, Lamb SE, Slowther AM, Woollard M, Carson A, et
al: Mechanical versus manual chest compression for out-of-hospital
cardiac arrest (PARAMEDIC): A pragmatic, cluster randomised
controlled trial. Lancet. 385:947–955. 2015.PubMed/NCBI View Article : Google Scholar
|
|
41
|
Newberry R, Redman T, Ross E, Ely R,
Saidler C, Arana A, Wampler D and Miramontes D: No benefit in
neurologic outcomes of survivors of out-of-hospital cardiac arrest
with mechanical compression device. Prehosp Emerg Care. 22:338–434.
2018.PubMed/NCBI View Article : Google Scholar
|
|
42
|
Hardig BM, Lindgren E, Östlund O, Herlitz
J, Karlsten R and Rubertsson S: Outcome among VF/VT patients in the
LINC (LUCAS IN cardiac arrest) trial-A randomised, controlled
trial. Resuscitation. 115:155–162. 2017.PubMed/NCBI View Article : Google Scholar
|
|
43
|
Ahn JY, Ryoo HW, Moon S, Jung H, Park J,
Lee WK, Kim JY, Lee DE, Kim JH and Lee SH: Prehospital factors
associated with out-of-hospital cardiac arrest outcomes in a
metropolitan city: A 4-year multicenter study. BMC Emerg Med.
23(125)2023.PubMed/NCBI View Article : Google Scholar
|
|
44
|
Anantharaman V, Ng BL, Ang SH, Lee CY,
Leong SH, Ong ME, Chua SJ, Rabind AC, Anjali NB and Hao Y: Prompt
use of mechanical cardiopulmonary resuscitation in out-of-hospital
cardiac arrest: The MECCA study report. Singapore Med J.
58:424–431. 2017.PubMed/NCBI View Article : Google Scholar
|
|
45
|
Kim HJ, Lee D, Moon HJ, Jeong D, Shin TY,
In Hong S and Lee HJ: Korean Cardiac Arrest Research Consortium
(KoCARC) Investigators. Real-world comparison between mechanical
and manual cardiopulmonary resuscitation during the COVID-19
pandemic. Am J Emerg Med. 76:217–224. 2024.PubMed/NCBI View Article : Google Scholar
|
|
46
|
Mastenbrook J, Redinger KE, Vos D and
Dickson C: Retrospective comparison of prehospital sustained return
of spontaneous circulation (ROSC) rates within a single basic life
support jurisdiction using manual vs lund university cardiac assist
system (LUCAS-2) mechanical cardiopulmonary resuscitation. Cureus.
14(e26131)2022.PubMed/NCBI View Article : Google Scholar
|
|
47
|
Halhalli HC, Şancı E and Uslu T: The
comparison of manual and mechanical chest compression on survival
and long-term neurological outcome of nontraumatic out-of-hospital
cardiac arrest patients. J Emerg Med. 59:680–686. 2020.PubMed/NCBI View Article : Google Scholar
|
|
48
|
Chen YR, Liao CJ, Huang HC, Tsai CH, Su
YS, Liu CH, Hsu CF and Tsai MJ: The effect of implementing
mechanical cardiopulmonary resuscitation devices on out-of-hospital
cardiac arrest patients in an urban city of Taiwan. Int J Environ
Res Public Health. 18(3636)2021.PubMed/NCBI View Article : Google Scholar
|
|
49
|
Casner M, Andersen D and Isaacs SM: The
impact of a new CPR assist device on rate of return of spontaneous
circulation in out-of-hospital cardiac arrest. Prehosp Emerg Care.
9:61–67. 2005.PubMed/NCBI View Article : Google Scholar
|
|
50
|
Schmidbauer S, Herlitz J, Karlsson T,
Axelsson C and Friberg H: Use of automated chest compression
devices after out-of-hospital cardiac arrest in Sweden.
Resuscitation. 120:95–102. 2017.PubMed/NCBI View Article : Google Scholar
|
|
51
|
Primi R, Bendotti S, Currao A, Sechi GM,
Marconi G, Pamploni G, Panni G, Sgotti D, Zorzi E, Cazzaniga M, et
al: Use of mechanical chest compression for resuscitation in
out-of-hospital cardiac arrest-device matters: A
propensity-score-based match analysis. J Clin Med.
12(4429)2023.PubMed/NCBI View Article : Google Scholar
|
|
52
|
Jin K, Fu Y, Yin L, Yu S, Zhang L, Wang Y,
Zhu H, Xu J and Yu X: Influence factors analysis of mechanical
compression and hands-only compression on restoration of
spontaneous circulation and prognosis in patients with cardiac
arrest. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 31:303–308.
2019.PubMed/NCBI View Article : Google Scholar : (In Chinese).
|
|
53
|
Maule Y: Mechanical external chest
compression: A new adjuvant technology in cardiopulmonary
resuscitation. Urgences Accueil. 7:4–7. 2007.
|
|
54
|
Ong ME, Ornato JP, Edwards DP, Dhindsa HS,
Best AM, Ines CS, Hickey S, Clark B, Williams DC, Powell RG, et al:
Use of an automated, load-distributing band chest compression
device for out-of-hospital cardiac arrest resuscitation. JAMA.
295:2629–2637. 2006.PubMed/NCBI View Article : Google Scholar
|
|
55
|
Swanson M, Poniatowski M, O'Keefe M and
Springer P: A CPR assist device increased emergency department
admission and end tidal carbon dioxide partial pressures during
treatment of out of hospital cardiac arrest. Circulation.
114(554)2006.
|
|
56
|
Lairet JR and Lee M: A comparison of
standard manual cardiopulmonary resuscitation versus the Autopulse
mechanical cardiopulmonary resuscitation device. Ann Emerg Med. 46
(Suppl)(S114)2005.
|
|
57
|
Ornato JP, Peberdy MA, Edwards DP, et al:
Improvement in field return of spontaneous circulation using
circumferential chest compression cardiopulmonary resuscitation.
Prehosp Emerg Care. 9(104)2005.
|
|
58
|
de Wilde R, vd Weijden P, de Haan M, Bosch
J, de Nooij J and Harinck HIJ: ROSC at hospital admission in out of
hospital cardiac arrest using LUCAS. Resuscitation. 77
(Suppl)(S49)2008.
|
|
59
|
Paradis NA, Kamlan D, Ghilarducci D and
Palazzolo J: The California AutoPulse quality assurance registry.
Circulation. 120(S1457)2009.
|
|
60
|
Truhlar A, Hejna P, Zabka L, Zatopkova L
and Cerny V: Injuries caused by the autopulse and LUCAS II
resuscitation systems compared to manual chest compressions.
Resuscitation. 81 (Suppl)(S62)2010.
|
|
61
|
Morozov SN, Abdusalamov SN and Fedorov AY:
Improved prognosis after implementation of chest compression device
in out-of-hospital cardiac arrest. Eur Heart J. 3(S702)2012.
|
|
62
|
Liu Y: Two kinds of external chest
compression mode for out-of-hospital cardiac arrest patients
pressure quality effect analysis (Chinese). Chin J Emerg Disaster
Med. 10:657–659. 2016.
|
|
63
|
Canakci ME, Parpucu Bagceci K, Acar N,
Ozakin E, Baloglu Kaya F, Kuas C, Çetin M, Tiryaki Baştuğ B and
Karakılıç ME: Computed tomographic findings of injuries after
mechanical and manual resuscitation: A retrospective study. Cureus.
13(e15131)2021.PubMed/NCBI View Article : Google Scholar
|
|
64
|
Takayama W, Endo A, Morishita K and Otomo
Y: Manual chest compression versus automated chest compression
device during day-time and night-time resuscitation following
out-of-hospital cardiac arrest: A retrospective historical control
study. J Pers Med. 13(1202)2023.PubMed/NCBI View Article : Google Scholar
|
|
65
|
Viniol S, Thomas RP, Gombert S, König AM,
Betz S and Mahnken AH: Comparison of different resuscitation
methods with regard to injury patterns in cardiac arrest survivors
based on computer tomography. Eur J Radiol.
131(109244)2020.PubMed/NCBI View Article : Google Scholar
|
|
66
|
Saleem S, Sonkin R, Sagy I, Strugo R,
Jaffe E, Drescher M and Shiber S: Traumatic injuries following
mechanical versus manual chest compression. Open Access Emerg Med.
14:557–562. 2022.PubMed/NCBI View Article : Google Scholar
|
|
67
|
Lu XG, Kang X and Gong DB: The clinical
efficacy of Thumper modal 1007 cardiopulmonary resuscitation: A
prospective randomized control trial. Zhongguo Wei Zhong Bing Ji
Jiu Yi Xue. 22:496–497. 2010.PubMed/NCBI
|
|
68
|
Kuschner CE and Becker LB: Recent advances
in personalizing cardiac arrest resuscitation. F1000Res 8: F1000
Faculty Rev-915, 2019.
|
|
69
|
Wang PL and Brooks SC: Mechanical versus
manual chest compressions for cardiac arrest. Cochrane Database
Syst Rev. 8(CD007260)2018.PubMed/NCBI View Article : Google Scholar
|
|
70
|
Lazzarin T, Tonon CR, Martins D, Fávero EL
Jr, Baumgratz TD, Pereira FWL, Pinheiro VR, Ballarin RS, Queiroz
DAR, Azevedo PS, et al: Post-cardiac arrest: Mechanisms,
management, and future perspectives. J Clin Med.
12(259)2022.PubMed/NCBI View Article : Google Scholar
|
|
71
|
Nikolovski SS, Lazic AD, Fiser ZZ,
Obradovic IA, Tijanic JZ and Raffay V: Recovery and survival of
patients after out-of-hospital cardiac arrest: A literature review
showcasing the big picture of intensive care unit-related factors.
Cureus. 16(e54827)2024.PubMed/NCBI View Article : Google Scholar
|