Cancer is a major challenge to human health
worldwide, and, while making some progress, traditional cancer
treatments, such as chemotherapy, radiotherapy and surgery, often
have a series of limitations and side effects (1). However, in recent years, chimeric
antigen receptor (CAR)-T cell therapy, which is also known as the
‘living drug’, has emerged (2).
CAR-T cell therapy has garnered interest in the
field of cancer treatment as a personalized cancer immunotherapy
strategy (2,3). It works by altering the immune system
of a patient, allowing it to recognize, attack and remove cancer
cells (4). Among the immune
system, CAR-T cells are a special subpopulation of T cells that are
genetically engineered to express specific antigen receptors, and
to effectively recognize and destroy cancer cells (5). However, this therapy also faces
multifaceted challenges, such as antigen selection, treatment
tolerance and safety (6,7). Tumor cells lacking specific antigens
or displaying heterogeneity in antigen expression can impair the
antigen selectivity of CAR-T cells (8). Moreover, tumor cells can develop
resistance by downregulating antigen expression and enhancing the
activity of immune inhibitory factors in response to CAR-T
cell-induced cytotoxicity (9).
Additionally, cytokine release syndrome (CRS) induced by CAR-T cell
therapy, which manifests as fever and difficulty breathing, low
blood pressure, nausea and vomiting, poses a notable safety
challenge. Currently, progress has been made in addressing the
aforementioned issues by examining multiple antigen targets,
improving the design of CAR-T cells, adjusting drug dosages and
enhancing the activity of CAR-T cells. However, these measures have
not completely eliminated the challenges (9). Further research and efforts are
required to solve these problems, and to improve the efficacy and
safety of CAR-T cell therapy (10). It is hypothesized that with the
continuous progression of science and technology, CAR-T cell
therapy will serve an important role in the future and bring a
revolutionary change in individualized cancer treatment.
Currently, the majority of review articles primarily
focus on the side effects of CAR-T cell therapy, targeted therapies
for solid tumors, current limitations and novel structural designs
of CAR-T, providing a detailed and in-depth analysis and commentary
on these aspects. However, there is a lack of comprehensive
description of CAR-T cell therapy as a whole (4,11–13).
Therefore, by summarizing the recent literature on CAR-T cell
therapy, the present review provides a more comprehensive overview
of the latest research status of CAR-T cell therapy in terms of the
basic structure of CAR-T cells, the tumor-killing mechanism,
clinical treatment steps, an overview of the current stage of
clinical use and overview of marketed drugs, with an aim to assist
researchers in quickly and comprehensively understanding the latest
advancements in this field.
CAR-T cells are genetically modified T cells that
express the CAR protein on their surface (14). The CAR protein is composed of an
external recognition region and an internal signaling region
(6). The external recognition
region usually consists of a single-chain antibody (scFv) or
antigen-binding domain that recognizes and binds to specific
antigens on the surface of the target cancer cells (15). This recognition region can be
genetically engineered to ensure that it binds the target antigen
efficiently (16). The internal
signaling region typically includes the signaling molecules and
signaling modules required to activate T cells (6). When the CAR binds to the target
antigen, the internal signaling region initiates signaling that
prompts antigen-specific activation and proliferation of the CAR-T
cell (17).
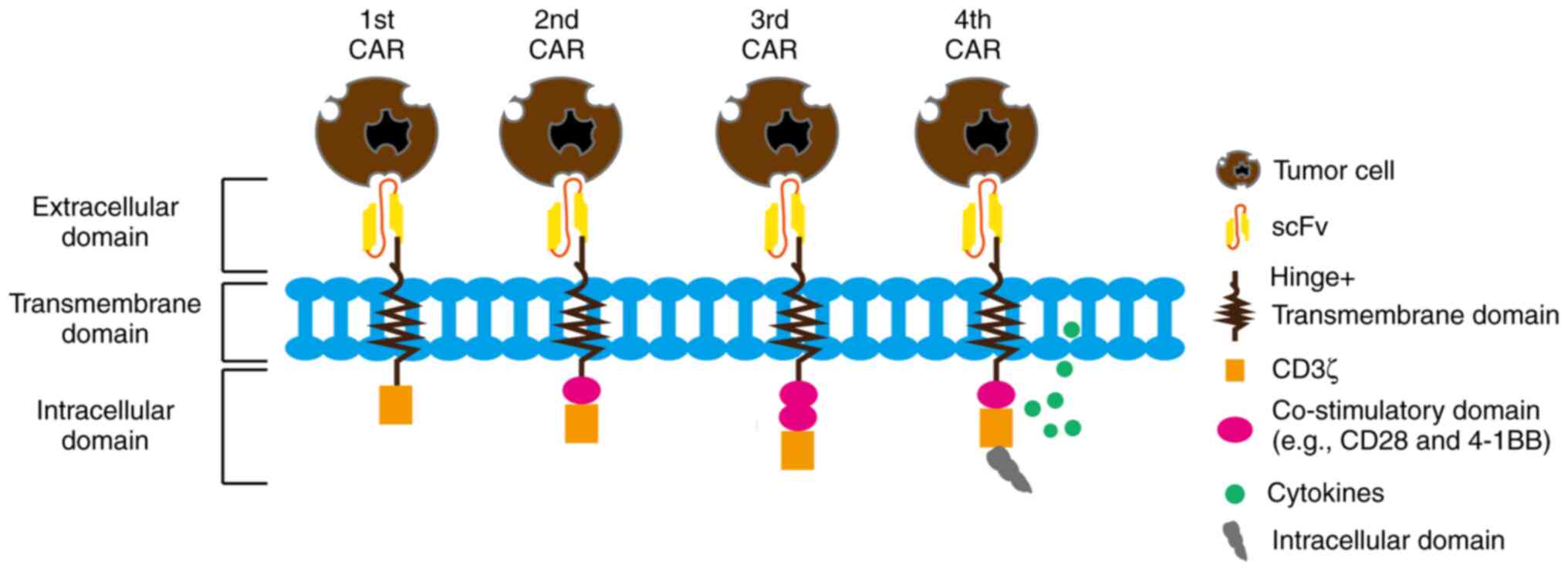
First-generation CARs typically contain an antigen
recognition domain and a CD3ζ transduction domain (9). This simple structure provides only
preliminary antigen recognition and T-cell activation signals
(29), but has a limited effect
and poor therapeutic efficacy for antigens with low-level
expression and heterogeneous expression (30). To enhance the activation and
persistence of CAR-T cells (31),
and to improve the therapeutic efficacy, studies introduced
second/third generation CARs (31,32).
The second-generation CARs have the addition of one or more
co-stimulatory factor domains, such as CD28 or 4-1BB, to the first
generation in order to enhance T-cell activation and to improve
cell proliferation and survival (31). The third-generation CARs have the
addition of further co-stimulatory factor domains to the second
generation (32). The
fourth-generation CARs exhibit an improved CAR structure via the
introduction of one or more stimulatory secretion cassettes or
polyclonal antibody secretion systems (33). These additional secretion elements
can secrete specific cytokines, such as IL-12 and IL-18, upon the
binding of CAR-T cells to antigens, further enhancing T-cell
activation and promoting the immune response and antitumor effects
(34,35). To increase the initial activation
state of CAR-T cells, preactivation domains, such as CD28 or CD137
preactivation domains, have been introduced in a number of CAR
designs (36–38). These domains enhance the activation
of CAR-T cells to a more favorable state prior to antigen binding
(39). To avoid cross-reactivity
with similar antigenic structures present in normal tissues,
studies have begun designing CAR-T cells with narrower antigen
recognition capabilities (39,40).
Restricted antigen recognition domains are achieved by selecting
specific fragile tumor-specific antigens or tumor-specific
neoantigens to improve therapeutic efficacy and reduce adverse
effects (40). These improved CAR
designs aim to increase CAR-T-cell persistence, enhance
cell-killing capacity and antitumor response, avoid unwanted
toxicity, and improve selective and specific recognition (41). Furthermore, the improved designs
can enhance cell proliferation and survival signaling, attenuate
activation-induced inhibitory signaling and promote memory T-cell
formation (Fig. 1) (42).
First, doctors screen patients to determine if the
patients are eligible to receive CAR-T cell therapy (51). This typically includes evaluating
the disease type, stage of disease, physical health and immune
system status of the patient (52). The peripheral blood of the patient
is collected, and the T cells are isolated using centrifugation and
immunomagnetic bead assay. In the laboratory, the T cells are
genetically modified to introduce the CAR gene, which enables the T
cells to recognize and attack specific tumor cells. The modified T
cells are expanded and cultured in vitro to increase their
number, which allows a sufficient number of CAR-T cells to be
obtained for use in therapy (53).
Before a patient receives CAR-T cell therapy, they may need to
undergo treatment preparation, such as lymphodepletion and bridging
therapy. Lymphodepletion is the conditioning treatment required for
CAR-T cell therapy and the goal of this therapy is to reduce
competing cell populations (including normal T cells, natural
killer cells and macrophages) in the patient and increase the
survival and therapeutic efficacy of the CAR-T cells (54). The number of immune cells in the
body is reduced using chemotherapy drugs or radiation therapy.
However, this approach has certain side effects, including
temporarily weakening the immune response of the patient and
increasing the risk of infection. Therefore, it is necessary to
administer antibiotics to prevent bacterial infections and to
monitor and treat any potential signs of infection in the patient
(53). Bridging therapy often
refers to the use of other treatments such as chemotherapy,
targeted therapy or radiation therapy before CAR-T cell therapy, in
order to control tumor progression or provide temporary therapeutic
effects. The purpose of bridge therapy is to buy time for patients
while waiting for the preparation and production of CAR-T cell
therapy (54). Once the CAR-T
cells are expanded to a sufficient number and the patient is
prepared for treatment, the doctor injects the CAR-T cells into the
patient through an intravenous infusion (55). Patients are closely observed and
monitored after receiving CAR-T cell therapy; this includes
monitoring for adverse reactions, evaluation of tumor response and
monitoring CAR-T cell activity and survival in the body (55).
During the CAR-T therapy process, there are also a
number of challenges in collecting T cells from the patient, and
the key to manufacturing CAR-T cells lies in appropriate T cell
collection and engineering. However, there may be manufacturing
failures due to poor sample quality, low cell quantity or
inadequate cell yield, and for certain patients with cancer, the
suppression of their own immune system can lead to a reduction in
the quantity or to an impairment of the function of the T cells in
the patient (56). During the
process of cell collection, external contamination from
microorganisms, bacteria, viruses and other contaminants may occur.
These contaminants can have a negative impact on the survival and
function of CAR-T cells, leading to a decrease in their quality
(54). Additionally, physical and
chemical damage may be inflicted on the cells during separation,
culture or transportation. Such damage can result in a decline in
cell function or even cell death, ultimately affecting the
therapeutic efficacy of the CAR-T cells (57–59).
This can lead to delays in starting treatment and increase the
difficulty and uncertainty of therapy. Manufacturing CAR-T cells
requires a certain amount of time to expand the cells and test
their quality. Typically, patients need to undergo other forms of
treatment during the waiting period, which can increase burdens,
require further medical resources and incur additional costs
(60).
CAR-T cell therapy has achieved notable application
results in hematological tumors (61). For example, CAR-T cells designed
against the CD19 antigen have achieved therapeutic effects by
targeting and killing CD19+ leukemia cells (62). In addition, CAR-T cell therapy has
shown notable efficacy in the treatment of relapsed/refractory
B-cell non-Hodgkin's lymphoma (B-NHL) (63), B-cell acute lymphoblastic leukemia
(B-ALL) and chronic lymphocytic leukemia, with ~40–60% of patients
with B-NHL obtaining durable remission and survival after receiving
CAR-T cell therapy, and ~80–90% of patients with B-ALL obtaining
durable remission and survival or complete remission, after
receiving CAR-T cell therapy (55,64).
The application of CAR-T cell therapy in the treatment of solid
tumors, as opposed to hematological tumors, continues to be
investigated, and despite a number of challenges and limitations,
positive advances have been made (65). CAR-T cells have been designed and
applied to target antigens on the cell surface of neuroblastoma
cells, such as GD2 (66).
Preliminary clinical trial data have shown that CAR-T cells
demonstrate some therapeutic efficacy in patients with high-risk
and refractory neuroblastoma (6).
CAR-T cells for prostate-specific memory acid phosphatase have also
demonstrated some anti-prostate cancer efficacy, and clinical
trials of CAR-T cell therapy for soft-tissue sarcoma have suggested
some potential (67,68). CAR-T cell therapies in solid tumors
face a number of challenges, such as antigenic diversity, immune
escape due to the tumor microenvironment and achieving sufficient
proliferation and infiltration (32,65,69).
These factors limit the application of CAR-T cell therapy in the
treatment of solid tumors (65).
Although CAR-T cell therapy has shown notable
efficacy in the treatment of hematological and solid tumors, it has
also brought about a number of treatment-associated side effects
and safety issues, and still faces a number of challenges in
clinical application that may limit its widespread use (65).
CRS is one of the most common side effects
associated with CAR-T cell therapy with an incidence of 20–50%
(70). When CAR-T cells kill tumor
cells, they release large amounts of cytokines, leading to the
overactivation of the immune system and systemic inflammatory
response (71,72). Mild CRS may manifest as symptoms
such as fever, chills and headache, while severe CRS may lead to
life-threatening conditions, such as hypotension, respiratory
distress and organ insufficiency (73). In addition, CAR-T cells exhibit
persistent cell proliferation, which can lead to organ function
impairment, and CRS may also cause anemia, thrombocytopenia and
leukopenia, which can induce spontaneous bleeding and increase the
risk of infection (74). The
release of cytokines can lead to a reduction in the number of
lymphocytes and other immune cells in the immune system (53). This lymphodepletion results in an
overall decrease in immune cells, including T cells, B cells and NK
cells, leading to cytopenia (75).
Additionally, the depletion of precursor cells in the hematopoietic
system can reduce the production of mature red blood cells, white
blood cells and platelets (75).
Headache, coma and neurological dysfunction are also possible side
effects (76). Furthermore, CAR-T
cells may have on-target off-tumor effects when CAR-T cells attack
non-tumor cells expressing the target antigen, but cells that do
not express this antigen are spared (71). Non-specific effects of CAR-T cell
therapy are likely due to inflammatory responses that can be
activated by CAR-T cell therapy (26).
The efficacy of CAR-T cell therapy is limited by the
selection and heterogeneity of target tumor antigens (77). Antigen expression varies between
tumor types and patients, and a number of tumors may even lack
specific antigens (78). In
addition, intratumor heterogeneity can make it more difficult for
CAR-T cells to recognize and attack antigens (79). Although CAR-T cell therapy has
resulted in long-term remission and survival in a number of
patients, not all patients will consistently benefit from this type
of therapy (80). Patients may
experience relapse or drug resistance, resulting in a less durable
efficacy after treatment (81).
Solid tumors typically have a complex tumor microenvironment,
including the production of immunosuppressive factors (such as
cytokines) and the interaction of tumor cells with other cells
(such as macrophages, regulatory T cells and myeloid suppressor
cells), so that the tumors may suppress the activity of CAR-T cells
32). This makes the infiltration and killing ability of CAR-T cells
in solid tumors limited, with a higher chance of immune escape
(42).
CAR-T cell therapy faces challenges in dealing with
tonic signaling, antigen loss and low antigen density (82). Tonic signaling refers to the state
where CAR-T cells remain active and release cytokines even in the
absence of normal stimulation, potentially leading to cytotoxicity
and unnecessary inflammation (83). Antigen loss occurs when tumor cells
lose the antigens originally targeted by CAR-T cells, rendering the
CAR-T cells unable to effectively kill these tumor cells, resulting
in treatment failure or relapse (84). Low antigen density is also a
notable challenge, as it means that there are fewer antigens on the
surface of target tumor cells. This low antigen density may prevent
CAR-T cells from accurately recognizing and attacking the target
cells, thereby reducing treatment efficacy (85). It has been revealed that by
improving the design of CAR-T cells and introducing switchable
activation technology, they can remain silent or regulate their
activity when lacking stimulation (22). To address the issues of antigen
loss and low antigen density, multi-antigen-targeting CAR-T cells
are being designed to simultaneously attack multiple antigens,
reducing the impact of losing a single antigen (82). Additionally, co-stimulatory
molecules are utilized to enhance CAR-T cell recognition and
cytotoxic activity against tumor cells (84). The phenotype and functional
characteristics of CAR-T cells is also affected by the selection of
the co-stimulatory domain (26).
Through pre-clinical investigations, the incorporation of a BBζ
co-stimulatory domain has been shown to preserve a greater
frequency of central memory CAR-T cells when compared with
CD28ζ-containing CAR-T cells, which were enriched for effector
memory phenotype cells (25,86).
However, this mainly applies to the second and third generation
CAR-T structure design. In comparison with terminally
differentiated effector cells, central memory CAR-T cells that have
been enriched with the BBζ co-stimulatory structural domain are
less differentiated and can give rise to daughter cells that
perform cytotoxic functions, whilst continuing to replenish the
population of memory cells for a longer response duration, thus
eliciting improved tumor control (86). Activation of the BB pathway has
been shown to promote T cell proliferation through the regulation
of cyclin-dependent kinases and to sustain the survival of
activated T cells. In trials involving patients with B cell
lymphoma subsets and chronic lymphocytic leukemia, the median
progression free survival of patients treated with CD28ζ CAR-T cell
products has in a number of cases spanned from 8–36 months
(84). Furthermore, there is
strong evidence in support of both CD28ζ and BBζ CAR-T cells, with
subsets of treated patients remaining in ongoing remission 7–10
years post-treatment (25,87). Analogous to investigations into BBζ
CAR-T cells, the addition of TNF-R superfamily molecules, such as
CD27 and OX40, in CAR design has led to improved antigen-dependent
memory formation and enhanced T cell survival (88).
Anti-BCMA CAR-T cell therapy is a targeted treatment
approach for multiple myeloma, a cancer of the plasma cells in bone
marrow (98). BCMA is an antigen
expressed on the surface of multiple myeloma cells and is
considered a critical therapeutic target for the disease (99). The therapy uses genetic engineering
techniques to modify the T cells of a patient to express CARs that
recognize and attack the BCMA (100). Currently, two anti-BCMA CAR-T
cell therapies (ide-cel and cilta-cel) have been approved by the
FDA for clinical treatment and have shown significant efficacy in
treating multiple myeloma (100).
The dosage and fractionation of CAR-T drugs are
crucial factors that can influence key aspects such as drug
efficacy and safety (98). The
dosage of CAT-T drugs is generally personalized based on factors
such as the weight and physical condition of the patient (98). Studies have revealed that anti-CD19
CAR-T cells achieved optimal clinical efficacy at a dose of 50–100
million cells/kg body weight, while anti-BCMA CAR-T cells
demonstrated optimal efficacy at a dose >100 million cells/kg
body weight, within a certain dose range (100,101). Increasing the dose may lead to an
increase in objective response rates (ORRs) until a threshold is
reached (98). However, when the
ORR begins to stabilize, further dose escalation is unlikely to
improve the ORR, but it may increase the incidence and/or severity
of adverse events associated with the mechanism (98). Excessive dosage can potentially
induce intense immune reactions and severe side effects, while
inadequate dosage may result in poor therapeutic outcomes (99). However, in a logistic regression
analysis concerning B-ALL, a higher CAR T-cell dose was associated
with a higher probability of response, there was no increase in CRS
incidence or severity across dose ranges and patients achieved
comparable early response rates independently of dose, but,
increasing the dose of CAR-T cells may lead to an increased risk of
CRS or neurotoxicity, which is a common concern (100). Further research is warranted to
elucidate the association between threshold dosing and post-CAR
outcomes (100). Therefore, a
comprehensive evaluation and personalized dosage adjustments are
necessary to achieve optimal treatment effects. Additionally, dose
fractionation is an important strategy for CAT-T drugs (100). Research has indicated that
treatment efficacy is not adversely affected by dose fractionation.
It has been suggested that, instead of a single dose infusion, dose
fractions of CAR-T cells administered over 2–3 days may decrease
the incidence and/or severity of CAR-T cell toxicity including CRS
and neurotoxicity, especially in patients with a high tumor burden
and for patients that require CAR-T cell therapy in higher doses
for efficacy (101). The effects
generated by a slow and continuous administration of drug often
exhibit longer-lasting and more stable outcomes compared with a
single high dose (101). This
approach involves dividing the drug into several equal parts and
administering them gradually over different time periods with the
aim to enhance treatment efficacy and reduce side effects (100). Dose stratification of CAR T-cell
treatment based on specific product characteristics or disease
burden, the use of phase I trial designs that incorporate efficacy
or pharmacokinetic data, and the development of CAR T-cells with
decreased potential for toxicity, could all aid clinicians and
researchers to optimize CAR T-cell dosing, expand the therapeutic
window and improve the availability of this emerging cancer
immunotherapy (99). These
strategies could also minimize drug toxicity and resistance as well
as reduce the frequency of adverse reactions during treatment.
At present, CAR-T cell therapy is mainly applied in
the treatment of certain hematological tumors. However, the future
development direction aims to expand the range of applications,
improve the therapeutic effects, reduce the serious side effects
and lower the cost of treatment (69). Studies are currently working on
further improvement measures to advance the effectiveness and
safety of CAR-T cell therapy (77,102). Potential measures include: i)
Introducing an adjustable switching system in order to start or
stop the activity of CAR-T cells in a timely manner to mitigate the
occurrence of adverse reactions (103); ii) exploring the use of multiple
CAR structures to recognize multiple antigens (104) or the use of bispecific CARs to
recognize two antigens at the same time to overcome immune escape
(105); iii) and utilizing gene
editing technology to precisely genetically modify CAR-T cells in
order to enhance their cellular activation, viability and antitumor
effects to mitigate antitumor immune escape mechanisms (106). Switching to CAR-NK cells, in
addition to T cells, may also be beneficial, as there is a class of
NK cells that also has antitumor effects (107). NK cells are one of the most
important cells in the immune system; CAR-NK cells, also known as
enhanced NK cells, can activate NK cells by breaking through the
limitations of killer immunoglobulin-like receptors, which are a
class of receptors expressed on the surface of NK cells that bind
to HLA-C-like molecules, thereby inhibiting NK cell activity, in
order to enhance the specific killing effect of NK cells on tumor
cells (108). Several factors in
the tumor microenvironment, such as immunosuppressive cells,
cytokines and infiltrating cells, may affect the function and
effectiveness of CAR-T cells (109). Therefore, studies are aiming to
enhance the survival and antitumor effects of CAR-T cells in the
tumor microenvironment using specific molecular targeting
strategies, such as receptors or antibodies on the surface of CAR-T
cells (9,102). These further improvements and
strategies are all aimed at further enhancing the efficacy,
durability and safety of CAR-T cell therapy. With in-depth research
on CAR-T cells and continuous technological innovations, it is
expected that CAR-T cell therapy will serve a greater role in the
field of cancer treatment in the future.
CAR-T cell therapy is a revolutionary immunotherapy
that has achieved notable success in treating a number of B
cell-associated malignancies. By targeting specific antigens on the
surface of tumors, CAR-T cells are able to identify and destroy
malignant cells, providing a new treatment option for those
patients for whom conventional therapies have failed. However,
CAR-T cell therapy still faces a number of challenges and
limitations. Serious adverse reactions, such as CRS and
neurotoxicity, may occur during treatment. By contrast, immune
escape mechanisms and suppression of the tumor microenvironment may
limit the effectiveness and durability of CAR-T cells. Therefore,
further improving the safety, specificity and durability of CAR-T
cell therapies is one of the current research priorities. In the
future, further development and application of CAR-T cell therapy
is expected. Firstly, the design and construction of CAR-T cells
will be continuously optimized, such as the introduction of
adjustable switch systems, bispecific CARs and genetically modified
CAR-T cells. Secondly, CAR-T cell therapy may be expanded to a
wider range of diseases, such as other types of cancer, autoimmune
diseases and infectious diseases. With the continuous research on
CAR-T cell therapy and technological advancement, the authors of
the present review are confident that CAR-T cell therapy will
continue to make progress in the future and serve an even greater
role in the field of cancer treatment and immune disease
therapy.
Not applicable.
The present review was funded by The Public Welfare Research
Project (Qianjiang, China; grant no. 2023GYX002).
Not applicable.
DS, XS, XY, SL and XW designed the theme of the
review; DS, XS, SL, XW, XY and MW retrieved the relevant
literature; and DS, XS, XY and MW wrote and reviewed the article.
Data authentication is not applicable. All authors read and
approved the final version of the manuscript.
Not applicable.
Not applicable.
The authors declare that they have no competing
interests.
|
1
|
Tsimberidou AM, Fountzilas E, Nikanjam M
and Kurzrock R: Review of precision cancer medicine: Evolution of
the treatment paradigm. Cancer Treat Rev. 86:1020192020. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Wu W, Zhou Q, Masubuchi T, Shi X, Li H, Xu
X, Huang M, Meng L, He X, Zhu H, et al: Multiple Signaling Roles of
CD3ε and Its Application in CAR-T Cell Therapy. Cell. 182:855–871.
e232020. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Parker KR, Migliorini D, Perkey E, Yost
KE, Bhaduri A, Bagga P, Haris M, Wilson NE, Liu F, Gabunia K, et
al: Single-Cell analyses identify brain mural cells expressing CD19
as Potential Off-Tumor Targets for CAR-T Immunotherapies. Cell.
183:126–142. e172020. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Sterner RC and Sterner RM: CAR-T cell
therapy: Current limitations and potential strategies. Blood Cancer
J. 11:692021. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Pan K, Farrukh H, Chittepu VCSR, Xu H, Pan
CX and Zhu Z: CAR race to cancer immunotherapy: From CAR T, CAR NK
to CAR macrophage therapy. J Exp Clin Cancer Res. 41:1192022.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Ahmad A: CAR-T Cell Therapy. Int J Mol
Sci. 21:43032020. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Feins S, Kong W, Williams EF, Milone MC
and Fraietta JA: An introduction to chimeric antigen receptor (CAR)
T-cell immunotherapy for human cancer. Am J Hematol. 94((S1)):
S3–S9. 2019.PubMed/NCBI
|
|
8
|
Majzner RG and Mackall CL: Tumor antigen
escape from CAR T-cell therapy. Cancer Discov. 8:1219–1226. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Abreu TR, Fonseca NA, Gonçalves N and
Moreira JN: Current challenges and emerging opportunities of CAR-T
cell therapies. J Control Release. 319:246–261. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Labanieh L, Majzner RG, Klysz D, Sotillo
E, Fisher CJ, Vilches-Moure JG, Pacheco KZB, Malipatlolla M, Xu P,
Hui JH, et al: Enhanced safety and efficacy of protease-regulated
CAR-T cell receptors. Cell. 185:1745–1763. e222022. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Flugel CL, Majzner RG, Krenciute G, Dotti
G, Riddell SR, Wagner DL and Abou-El-Enein M: Overcoming on-target,
off-tumour toxicity of CAR T cell therapy for solid tumours. Nat
Rev Clin Oncol. 20:49–62. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Chohan KL, Siegler EL and Kenderian SS:
CAR-T Cell Therapy: The efficacy and toxicity balance. Curr Hematol
Malig Rep. 18:9–18. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Chen YJ, Abila B and Mostafa Kamel Y:
CAR-T: What Is Next? Cancers (Basel). 15:6632023. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Schubert ML, Schmitt M, Wang L, Ramos CA,
Jordan K, Müller-Tidow C and Dreger P: Side-effect management of
chimeric antigen receptor (CAR) T-cell therapy. Ann Oncol.
32:34–48. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Bao C, Gao Q, Li LL, Han L, Zhang B, Ding
Y, Song Z, Zhang R, Zhang J and Wu XH: The application of nanobody
in CAR-T therapy. Biomolecules. 11:2382021. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Majzner RG, Rietberg SP, Sotillo E, Dong
R, Vachharajani VT, Labanieh L, Myklebust JH, Kadapakkam M, Weber
EW, Tousley AM, et al: Tuning the antigen density requirement for
CAR T-cell Activity. Cancer Discov. 10:702–723. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Depil S, Duchateau P, Grupp SA, Mufti G
and Poirot L: ‘Off-the-shelf’ allogeneic CAR T cells: development
and challenges. Nat Rev Drug Discov. 19:185–199. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Benmebarek MR, Karches CH, Cadilha BL,
Lesch S, Endres S and Kobold S: Killing mechanisms of chimeric
antigen receptor (CAR) T Cells. Int J Mol Sci. 20:12832019.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Rafiq S, Yeku OO, Jackson HJ, Purdon TJ,
van Leeuwen DG, Drakes DJ, Song M, Miele MM, Li Z, Wang P, et al:
Targeted delivery of a PD-1-blocking scFv by CAR-T cells enhances
anti-tumor efficacy in vivo. Nat Biotechnol. 36:847–856. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
van de Donk NWCJ, Usmani SZ and Yong K:
CAR T-cell therapy for multiple myeloma: State of the art and
prospects. Lancet Haematol. 8:e446–e461. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Srivastava S and Riddell SR: Engineering
CAR-T cells: Design concepts. Trends Immunol. 36:494–502. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Duan Y, Chen R, Huang Y, Meng X, Chen J,
Liao C, Tang Y, Zhou C, Gao X and Sun J: Tuning the ignition of
CAR: optimizing the affinity of scFv to improve CAR-T therapy. Cell
Mol Life Sci. 79:142021. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Weber EW, Parker KR, Sotillo E, Lynn RC,
Anbunathan H, Lattin J, Good Z, Belk JA, Daniel B, Klysz D, et al:
Transient rest restores functionality in exhausted CAR-T cells
through epigenetic remodeling. Science. 372:eaba17862021.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Tousley AM, Rotiroti MC, Labanieh L,
Rysavy LW, Kim WJ, Lareau C, Sotillo E, Weber EW, Rietberg SP,
Dalton GN, et al: Co-opting signalling molecules enables
logic-gated control of CAR T cells. Nature. 615:507–516. 2023.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Honikel MM and Olejniczak SH:
Co-Stimulatory receptor signaling in CAR-T Cells. Biomolecules.
12:13032022. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Huang R, Li X, He Y, Zhu W, Gao L, Liu Y,
Gao L, Wen Q, Zhong JF, Zhang C and Zhang X: Recent advances in
CAR-T cell engineering. J Hematol Oncol. 13:862020. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Singh N, Frey NV, Engels B, Barrett DM,
Shestova O, Ravikumar P, Cummins KD, Lee YG, Pajarillo R, Chun I,
et al: Antigen-independent activation enhances the efficacy of
4-1BB-costimulated CD22 CAR T cells. Nat Med. 27:842–850. 2021.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Smole A, Benton A, Poussin MA, Eiva MA,
Mezzanotte C, Camisa B, Greco B, Sharma P, Minutolo NG, Gray F, et
al: Expression of inducible factors reprograms CAR-T cells for
enhanced function and safety. Cancer Cell. 40:1470–1487. e772022.
View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Drougkas K, Karampinos K, Karavolias I,
Koumprentziotis IA, Ploumaki I, Triantafyllou E, Trontzas I and
Kotteas E: Comprehensive clinical evaluation of CAR-T cell
immunotherapy for solid tumors: A path moving forward or a dead
end? J Cancer Res Clin Oncol. 149:2709–2734. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Westin J and Sehn LH: CAR T cells as a
second-line therapy for large B-cell lymphoma: A paradigm shift?
Blood. 139:2737–2746. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Roselli E, Boucher JC, Li G, Kotani H,
Spitler K, Reid K, Cervantes EV, Bulliard Y, Tu N, Lee SB, et al:
4-1BB and optimized CD28 co-stimulation enhances function of human
mono-specific and bi-specific third-generation CAR T cells. J
Immunother Cancer. 9:e0033542021. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Martinez M and Moon EK: CAR T cells for
solid tumors: New strategies for finding, infiltrating, and
surviving in the tumor microenvironment. Front Immunol. 10:1282019.
View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Barros LRC, Couto SCF, da Silva Santurio
D, Paixão EA, Cardoso F, da Silva VJ, Klinger P, Ribeiro PDAC, Rós
FA, Oliveira TGM, et al: Systematic review of available CAR-T Cell
Trials around the World. Cancers (Basel). 14:26672022. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Agliardi G, Liuzzi AR, Hotblack A, De Feo
D, Núñez N, Stowe CL, Friebel E, Nannini F, Rindlisbacher L,
Roberts TA, et al: Intratumoral IL-12 delivery empowers CAR-T cell
immunotherapy in a pre-clinical model of glioblastoma. Nat Commun.
12:4442021. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Glienke W, Dragon AC, Zimmermann K,
Martyniszyn-Eiben A, Mertens M, Abken H, Rossig C, Altvater B,
Aleksandrova K, Arseniev L, et al: GMP-Compliant Manufacturing of
TRUCKs: CAR T Cells targeting GD(2) and Releasing Inducible IL-18.
Front Immunol. 13:8397832022. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Etxeberria I, Glez-Vaz J, Teijeira Á and
Melero I: New emerging targets in cancer immunotherapy: CD137/4-1BB
costimulatory axis. ESMO Open. 4 (Suppl 3):e0007332020. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Sanchez-Paulete AR, Labiano S,
Rodriguez-Ruiz ME, Azpilikueta A, Etxeberria I, Bolaños E, Lang V,
Rodriguez M, Aznar MA, Jure-Kunkel M and Melero I: Deciphering
CD137 (4-1BB) signaling in T-cell costimulation for translation
into successful cancer immunotherapy. Eur J Immunol. 46:513–522.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Liu Y, An L, Huang R, Xiong J, Yang H,
Wang X and Zhang X: Strategies to enhance CAR-T persistence.
Biomark Res. 10:862022. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Xiao Q, Zhang X, Tu L, Cao J, Hinrichs CS
and Su X: Size-dependent activation of CAR-T cells. Sci Immunol.
7:eabl39952022. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Zheng N, Fang J, Xue G, Wang Z, Li X, Zhou
M, Jin G, Rahman MM, McFadden G and Lu Y: Induction of tumor cell
autosis by myxoma virus-infected CAR-T and TCR-T cells to overcome
primary and acquired resistance. Cancer Cell. 40:973–985. e72022.
View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Brudno JN and Kochenderfer JN: Recent
advances in CAR T-cell toxicity: Mechanisms, manifestations and
management. Blood Rev. 34:45–55. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Boyiadzis MM, Dhodapkar MV, Brentjens RJ,
Kochenderfer JN, Neelapu SS, Maus MV, Porter DL, Maloney DG, Grupp
SA, Mackall CL, et al: Chimeric antigen receptor (CAR) T therapies
for the treatment of hematologic malignancies: Clinical perspective
and significance. J Immunother Cancer. 6:1372018. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Choi BD, Yu X, Castano AP, Bouffard AA,
Schmidts A, Larson RC, Bailey SR, Boroughs AC, Frigault MJ, Leick
MB, et al: CAR-T cells secreting BiTEs circumvent antigen escape
without detectable toxicity. Nat Biotechnol. 37:1049–1058. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Marei HE, Althani A, Afifi N, Hasan A,
Caceci T, Pozzoli G and Cenciarelli C: Current progress in chimeric
antigen receptor T cell therapy for glioblastoma multiforme. Cancer
Med. 10:5019–5030. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Zhu H, Fang X, Tuhin IJ, Tan J, Ye J, Jia
Y, Xu N, Kang L, Li M, Lou X, et al: CAR T cells equipped with a
fully human scFv targeting Trop2 can be used to treat pancreatic
cancer. J Cancer Res Clin Oncol. 148:2261–2274. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Feng Q, Sun B, Xue T, Li R, Lin C, Gao Y,
Sun L, Zhuo Y and Wang D: Advances in CAR T-cell therapy in bile
duct, pancreatic, and gastric cancers. Front Immunol.
13:10256082022. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Entezam M, Sanaei MJ, Mirzaei Y, Mer AH,
Abdollahpour-Alitappeh M, Azadegan-Dehkordi F and Bagheri N:
Current progress and challenges of immunotherapy in gastric cancer:
A focus on CAR-T cells therapeutic approach. Life Sci.
318:1214592023. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Davenport AJ, Jenkins MR, Cross RS, Yong
CS, Prince HM, Ritchie DS, Trapani JA, Kershaw MH, Darcy PK and
Neeson PJ: CAR-T cells inflict sequential killing of multiple tumor
target cells. Cancer Immunol Res. 3:483–494. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Chen C, Gu YM, Zhang F, Zhang ZC, Zhang
YT, He YD, Wang L, Zhou N, Tang FT, Liu HJ and Li YM: Construction
of PD1/CD28 chimeric-switch receptor enhances anti-tumor ability of
c-Met CAR-T in gastric cancer. Oncoimmunology. 10:19014342021.
View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Cohen AD, Garfall AL, Stadtmauer EA,
Melenhorst JJ, Lacey SF, Lancaster E, Vogl DT, Weiss BM, Dengel K,
Nelson A, et al: B cell maturation antigen-specific CAR T cells are
clinically active in multiple myeloma. J Clin Invest.
129:2210–2221. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Pasqui DM, Latorraca CDOC, Pacheco RL and
Riera R: CAR-T cell therapy for patients with hematological
malignancies. A systematic review. Eur J Haematol. 109:601–618.
2022. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Fabrizio VA, Boelens JJ, Mauguen A,
Baggott C, Prabhu S, Egeler E, Mavroukakis S, Pacenta H, Phillips
CL, Rossoff J, et al: Optimal fludarabine lymphodepletion is
associated with improved outcomes after CAR T-cell therapy. Blood
Adv. 6:1961–1968. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Bupha-Intr O, Haeusler G, Chee L, Thursky
K, Slavin M and The B: CAR-T cell therapy and infection: a review.
Expert Rev Anti Infect Ther. 19:749–758. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Roddie C, Neill L, Osborne W, Iyengar S,
Tholouli E, Irvine D, Chaganti S, Besley C, Bloor A, Jones C, et
al: Effective bridging therapy can improve CD19 CAR-T outcomes
while maintaining safety in patients with large B-cell lymphoma.
Blood Adv. 7:2872–2883. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
55
|
Mangal JL, Handlos JL, Esrafili A, Inamdar
S, Mcmillian S, Wankhede M, Gottardi R and Acharya AP: Engineering
metabolism of chimeric antigen receptor (CAR) cells for developing
efficient immunotherapies. Cancers (Basel). 13:11232021. View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Chow A, Perica K, Klebanoff CA and Wolchok
JD: Clinical implications of T cell exhaustion for cancer
immunotherapy. Nat Rev Clin Oncol. 19:775–790. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
57
|
Martino M, Alati C, Canale FA, Musuraca G,
Martinelli G and Cerchione C: A review of clinical outcomes of CAR
T-Cell Therapies for B-Acute lymphoblastic leukemia. Int J Mol Sci.
22:21502021. View Article : Google Scholar : PubMed/NCBI
|
|
58
|
Geldres C, Savoldo B and Dotti G: Chimeric
antigen receptor-redirected T cells return to the bench. Semin
Immunol. 28:3–9. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
59
|
Neelapu SS, Tummala S, Kebriaei P, Wierda
W, Gutierrez C, Locke FL, Komanduri KV, Lin Y, Jain N, Daver N, et
al: Chimeric antigen receptor T-cell therapy-assessment and
management of toxicities. Nat Rev Clin Oncol. 15:47–62. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
60
|
Zhang X, Zhang H, Lan H, Wu J and Xiao Y:
CAR-T cell therapy in multiple myeloma: Current limitations and
potential strategies. Front Immunol. 14:11014952023. View Article : Google Scholar : PubMed/NCBI
|
|
61
|
Haslauer T, Greil R, Zaborsky N and
Geisberger R: CAR T-Cell therapy in hematological malignancies. Int
J Mol Sci. 22:89962021. View Article : Google Scholar : PubMed/NCBI
|
|
62
|
Jin X, Xu Q, Pu C, Zhu K, Lu C, Jiang Y,
Xiao L, Han Y and Lu L: Therapeutic efficacy of anti-CD19 CAR-T
cells in a mouse model of systemic lupus erythematosus. Cell Mol
Immunol. 18:1896–1903. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
63
|
Denlinger N, Bond D and Jaglowski S: CAR
T-cell therapy for B-cell lymphoma. Curr Probl Cancer.
46:1008262022. View Article : Google Scholar : PubMed/NCBI
|
|
64
|
Shalabi H, Qin H, Su A, Yates B, Wolters
PL, Steinberg SM, Ligon JA, Silbert S, DéDé K, Benzaoui M, et al:
CD19/22 CAR T cells in children and young adults with B-ALL: Phase
1 results and development of a novel bicistronic CAR. Blood.
140:451–463. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
65
|
Ma S, Li X, Wang X, Cheng L, Li Z, Zhang
C, Ye Z and Qian Q: Current Progress in CAR-T cell therapy for
solid tumors. Int J Biol Sci. 15:2548–2560. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
66
|
Majzner RG, Ramakrishna S, Yeom KW, Patel
S, Chinnasamy H, Schultz LM, Richards RM, Jiang L, Barsan V,
Mancusi R, et al: GD2-CAR T cell therapy for H3K27M-mutated diffuse
midline gliomas. Nature. 603:934–941. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
67
|
Zarrabi KK, Narayan V, Mille PJ, Zibelman
MR, Miron B, Bashir B and Kelly WK: Bispecific PSMA antibodies and
CAR-T in metastatic castration-resistant prostate cancer. Ther Adv
Urol. 15:175628722311822192023. View Article : Google Scholar : PubMed/NCBI
|
|
68
|
Narayan V, Barber-Rotenberg JS, Jung IY,
Lacey SF, Rech AJ, Davis MM, Hwang WT, Lal P, Carpenter EL, Maude
SL, et al: PSMA-targeting TGFβ-insensitive armored CAR T cells in
metastatic castration-resistant prostate cancer: A phase 1 trial.
Nat Med. 28:724–734. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
69
|
Miller IC, Zamat A, Sun LK, Phuengkham H,
Harris AM, Gamboa L, Yang J, Murad JP, Priceman SJ and Kwong GA:
Enhanced intratumoural activity of CAR T cells engineered to
produce immunomodulators under photothermal control. Nat Biomed
Eng. 5:1348–1359. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
70
|
Hu Y, Li J, Ni F, Yang Z, Gui X, Bao Z,
Zhao H, Wei G, Wang Y, Zhang M, et al: CAR-T cell therapy-related
cytokine release syndrome and therapeutic response is modulated by
the gut microbiome in hematologic malignancies. Nat Commun.
13:53132022. View Article : Google Scholar : PubMed/NCBI
|
|
71
|
Giavridis T, van der Stegen SJC, Eyquem J,
Hamieh M, Piersigilli A and Sadelain M: CAR T cell-induced cytokine
release syndrome is mediated by macrophages and abated by IL-1
blockade. Nat Med. 24:731–738. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
72
|
Xiao X, Huang S, Chen S, Wang Y, Sun Q, Xu
X and Li Y: Mechanisms of cytokine release syndrome and
neurotoxicity of CAR T-cell therapy and associated prevention and
management strategies. J Exp Clin Cancer Res. 40:3672021.
View Article : Google Scholar : PubMed/NCBI
|
|
73
|
Xu J, Chen LJ, Yang SS, Sun Y, Wu W, Liu
YF, Xu J, Zhuang Y, Zhang W, Weng XQ, et al: Exploratory trial of a
biepitopic CAR T-targeting B cell maturation antigen in
relapsed/refractory multiple myeloma. Proc Natl Acad Sci USA.
116:9543–9551. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
74
|
Mei H, Li C, Jiang H, Zhao X, Huang Z, Jin
D, Guo T, Kou H, Liu L, Tang L, et al: A bispecific CAR-T cell
therapy targeting BCMA and CD38 in relapsed or refractory multiple
myeloma. J Hematol Oncol. 14:1612021. View Article : Google Scholar : PubMed/NCBI
|
|
75
|
Jain T, Olson TS and Locke FL: How I treat
cytopenias after CAR T-cell therapy. Blood. 141:2460–2469.
2023.PubMed/NCBI
|
|
76
|
Gust J, Hay KA, Hanafi LA, Li D, Myerson
D, Gonzalez-Cuyar LF, Yeung C, Liles WC, Wurfel M, Lopez JA, et al:
Endothelial activation and blood-brain barrier disruption in
neurotoxicity after adoptive immunotherapy with CD19 CAR-T Cells.
Cancer Discov. 7:1404–1419. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
77
|
Corti C, Venetis K, Sajjadi E, Zattoni L,
Curigliano G and Fusco N: CAR-T cell therapy for triple-negative
breast cancer and other solid tumors: preclinical and clinical
progress. Expert Opin Investig Drugs. 31:593–605. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
78
|
Zhang J, Hu Y, Yang J, Li W, Zhang M, Wang
Q, Zhang L, Wei G, Tian Y, Zhao K, et al: Non-viral, specifically
targeted CAR-T cells achieve high safety and efficacy in B-NHL.
Nature. 609:369–374. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
79
|
Mensali N, Köksal H, Joaquina S, Wernhoff
P, Casey NP, Romecin P, Panisello C, Rodriguez R, Vimeux L,
Juzeniene A, et al: ALPL-1 is a target for chimeric antigen
receptor therapy in osteosarcoma. Nat Commun. 14:33752023.
View Article : Google Scholar : PubMed/NCBI
|
|
80
|
Cappell KM and Kochenderfer JN: Long-term
outcomes following CAR T cell therapy: What we know so far. Nat Rev
Clin Oncol. 20:359–371. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
81
|
Shah NN and Fry TJ: Mechanisms of
resistance to CAR T cell therapy. Nat Rev Clin Oncol. 16:372–385.
2019.PubMed/NCBI
|
|
82
|
Jayaraman J, Mellody MP, Hou AJ, Desai RP,
Fung AW, Pham AHT, Chen YY and Zhao W: CAR-T design: Elements and
their synergistic function. EBioMedicine. 58:1029312020. View Article : Google Scholar : PubMed/NCBI
|
|
83
|
Chen J, Qiu S, Li W, Wang K, Zhang Y, Yang
H, Liu B, Li G, Li L, Chen M, et al: Tuning charge density of
chimeric antigen receptor optimizes tonic signaling and CAR-T cell
fitness. Cell Res. 33:341–354. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
84
|
Hamieh M, Dobrin A, Cabriolu A, van der
Stegen SJC, Giavridis T, Mansilla-Soto J, Eyquem J, Zhao Z,
Whitlock BM, Miele MM, et al: CAR T cell trogocytosis and
cooperative killing regulate tumour antigen escape. Nature.
568:112–116. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
85
|
Heitzeneder S, Bosse KR, Zhu Z, Zhelev D,
Majzner RG, Radosevich MT, Dhingra S, Sotillo E, Buongervino S,
Pascual-Pasto G, et al: GPC2-CAR T cells tuned for low antigen
density mediate potent activity against neuroblastoma without
toxicity. Cancer Cell. 40:53–69.e9. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
86
|
Ramos CA, Rouce R, Robertson CS, Reyna A,
Narala N, Vyas G, Mehta B, Zhang H, Dakhova O, Carrum G, et al: In
Vivo Fate and Activity of Second-versus Third-Generation
CD19-Specific CAR-T Cells in B Cell Non-Hodgkin's Lymphomas. Mol
Ther. 26:2727–2737. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
87
|
Turtle CJ, Hanafi LA, Berger C, Gooley TA,
Cherian S, Hudecek M, Sommermeyer D, Melville K, Pender B, Budiarto
TM, et al: CD19 CAR-T cells of defined CD4+:CD8+ composition in
adult B cell ALL patients. J Clin Invest. 126:2123–2138. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
88
|
Song DG, Ye Q, Poussin M, Harms GM, Figini
M and Powell DJ Jr: CD27 costimulation augments the survival and
antitumor activity of redirected human T cells in vivo. Blood.
119:696–706. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
89
|
Bachy E, Le Gouill S, Di Blasi R, Sesques
P, Manson G, Cartron G, Beauvais D, Roulin L, Gros FX, Rubio MT, et
al: A real-world comparison of tisagenlecleucel and axicabtagene
ciloleucel CAR T cells in relapsed or refractory diffuse large B
cell lymphoma. Nat Med. 28:2145–2154. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
90
|
Han D, Xu Z, Zhuang Y, Ye Z and Qian Q:
Current Progress in CAR-T cell therapy for hematological
malignancies. J Cancer. 12:326–334. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
91
|
Siddiqi T, Soumerai JD, Dorritie KA,
Stephens DM, Riedell PA, Arnason J, Kipps TJ, Gillenwater HH, Gong
L, Yang L, et al: Phase 1 TRANSCEND CLL 004 study of lisocabtagene
maraleucel in patients with relapsed/refractory CLL or SLL. Blood.
139:1794–1806. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
92
|
Feng D and Sun J: Overview of anti-BCMA
CAR-T immunotherapy for multiple myeloma and relapsed/refractory
multiple myeloma. Scand J Immunol. 92:e129102020. View Article : Google Scholar : PubMed/NCBI
|
|
93
|
Raje N, Berdeja J, Lin Y, Siegel D,
Jagannath S, Madduri D, Liedtke M, Rosenblatt J, Maus MV, Turka A,
et al: Anti-BCMA CAR T-Cell Therapy bb2121 in Relapsed or
Refractory Multiple Myeloma. N Engl J Med. 380:1726–1737. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
94
|
Curran E and O'Brien M: Role of
blinatumomab, inotuzumab, and CAR T-cells: Which to choose and how
to sequence for patients with relapsed disease. Semin Hematol.
57:157–163. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
95
|
Fry TJ, Shah NN, Orentas RJ,
Stetler-Stevenson M, Yuan CM, Ramakrishna S, Wolters P, Martin S,
Delbrook C, Yates B, et al: CD22-targeted CAR T cells induce
remission in B-ALL that is naive or resistant to CD19-targeted CAR
immunotherapy. Nat Med. 24:20–28. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
96
|
Xu J, Meng Q, Sun H, Zhang X, Yun J, Li B,
Wu S, Li X, Yang H, Zhu H, et al: HER2-specific chimeric antigen
receptor-T cells for targeted therapy of metastatic colorectal
cancer. Cell Death Dis. 12:11092021. View Article : Google Scholar : PubMed/NCBI
|
|
97
|
Maggs L, Cattaneo G, Dal AE, Moghaddam AS
and Ferrone S: CAR T Cell-Based immunotherapy for the treatment of
glioblastoma. Front Neurosci. 15:6620642021. View Article : Google Scholar : PubMed/NCBI
|
|
98
|
Rotte A, Frigault MJ, Ansari A, Gliner B,
Heery C and Shah B: Dose-response correlation for CAR-T cells: A
systematic review of clinical studies. J Immunother Cancer.
10:e0056782022. View Article : Google Scholar : PubMed/NCBI
|
|
99
|
Dasyam N, George P and Weinkove R:
Chimeric antigen receptor T-cell therapies: Optimising the dose. Br
J Clin Pharmacol. 86:1678–1689. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
100
|
Stefanski HE, Eaton A, Baggott C, Rossoff
J, Verneris MR, Prabhu S, Pacenta HL, Phillips CL, Talano JA,
Moskop A, et al: Higher doses of tisagenlecleucel are associated
with improved outcomes: A report from the pediatric real-world CAR
consortium. Blood Adv. 7:541–548. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
101
|
Frigault M, Rotte A, Ansari A, Gliner B,
Heery C and Shah B: Dose fractionation of CAR-T cells. A systematic
review of clinical outcomes. J Exp Clin Cancer Res. 42:112023.
View Article : Google Scholar : PubMed/NCBI
|
|
102
|
Jogalekar MP, Rajendran RL, Khan F, Dmello
C, Gangadaran P and Ahn BC: CAR T-Cell-Based gene therapy for
cancers: New perspectives, challenges, and clinical developments.
Front Immunol. 13:9259852022. View Article : Google Scholar : PubMed/NCBI
|
|
103
|
Wagner DL, Koehl U, Chmielewski M, Scheid
C and Stripecke R: Review: Sustainable Clinical Development of
CAR-T Cells-switching from viral transduction towards CRISPR-Cas
Gene Editing. Front Immunol. 13:8654242022. View Article : Google Scholar : PubMed/NCBI
|
|
104
|
Gagelmann N, Riecken K, Wolschke C, Berger
C, Ayuk FA, Fehse B and Kröger N: Development of CAR-T cell
therapies for multiple myeloma. Leukemia. 34:2317–2332. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
105
|
Zeng W, Zhang Q, Zhu Y, Ou R, Peng L, Wang
B, Shen H, Liu Z, Lu L, Zhang P and Liu S: Engineering Novel
CD19/CD22 Dual-Target CAR-T cells for improved anti-tumor activity.
Cancer Invest. 40:282–292. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
106
|
Ghaffari S, Khalili N and Rezaei N:
CRISPR/Cas9 revitalizes adoptive T-cell therapy for cancer
immunotherapy. J Exp Clin Cancer Res. 40:2692021. View Article : Google Scholar : PubMed/NCBI
|
|
107
|
Hong M and Chen YY: Killer fatigue:
Transition to NK-cell-like phenotype is a signature of CAR-T cell
exhaustion. Cell. 184:6017–6019. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
108
|
Good CR, Aznar MA, Kuramitsu S, Samareh P,
Agarwal S, Donahue G, Ishiyama K, Wellhausen N, Rennels AK, Ma Y,
et al: An NK-like CAR T cell transition in CAR T cell dysfunction.
Cell. 184:6081–6100. e262021. View Article : Google Scholar : PubMed/NCBI
|
|
109
|
Allen GM, Frankel NW, Reddy NR, Bhargava
HK, Yoshida MA, Stark SR, Purl M, Lee J, Yee JL, Yu W, et al:
Synthetic cytokine circuits that drive T cells into immune-excluded
tumors. Science. 378:eaba16242022. View Article : Google Scholar : PubMed/NCBI
|