Introduction
Perivascular epithelioid cells (PECs) were first
proposed in 1992 by Bonetti et al(1) and classified by the World Health
Organization in 2002 (2,3). The PEC tumor (PEComa) family is
composed of epithelioid angiomyolipoma (AML), clear-cell ‘sugar’
tumors, lymphangioleiomyomatosis, clear-cell myomelanocytic tumors
of the falciform ligament/ligamentum teres and rare clear-cell
tumors of other anatomical sites (4–6).
PEComa is mainly composed of eosinophilic and clear epithelioid
cells, which are commonly arranged as small nests that are
associated with variably-sized vessels (5–7). The
predominant site of origin for PEComa is the uterus, but the tumor
may also be found in the falciform ligaments, prostate and kidney.
However, cases in the liver are extremely rare (2,8).
Hepatic PEComa has a marked female predominance and possesses no
specific symptoms (9). The
diagnosis of PEComa is based on its pathological characteristics,
including epithelioid cells without adipocytes or abnormal blood
vessels, and on immunohistochemical evidence, including melanocytic
and smooth muscle markers (8).
Surgery is the only effective method to result in a long survival
time (6,9).
In the present study, one case of hepatic PEComa is
described. Furthermore, 19 cases from the literature, in which 11
patients were diagnosed with hepatic PEComa and eight with hepatic
epithelioid angiomyolipoma, are reviewed.
Case report
Presentation and laboratory
examinations
A 25-year-old female who presented with an abdominal
mass, which was revealed by ultrasonography, was admitted to the
Second Affiliated Hospital, Zhejiang University School of Medicine
(Zhejiang, Hangzhou, China) in December 2011. The past history and
physical examination were normal. The laboratory examinations
revealed a slightly elevated level of carbohydrate antigen 19-9
(CA199; 38.8 kU/l; reference range, <37 kU/l). The levels of
alanine aminotransferase (ALT; 7 U/l), aspartate aminotransferase
(AST; 14 U/l), serum creatinine (SCr; 49 μmol/l), blood urea
nitrogen (BUN; 3.80 mmol/l), α-fetoprotein (AFP; 2.2 μg/l) and
carcinoembryonic antigen (CEA; 0.9 μg/l) were within the reference
ranges. Hepatitis B and hepatitis C virus screenings were
negative.
Diagnostic techniques
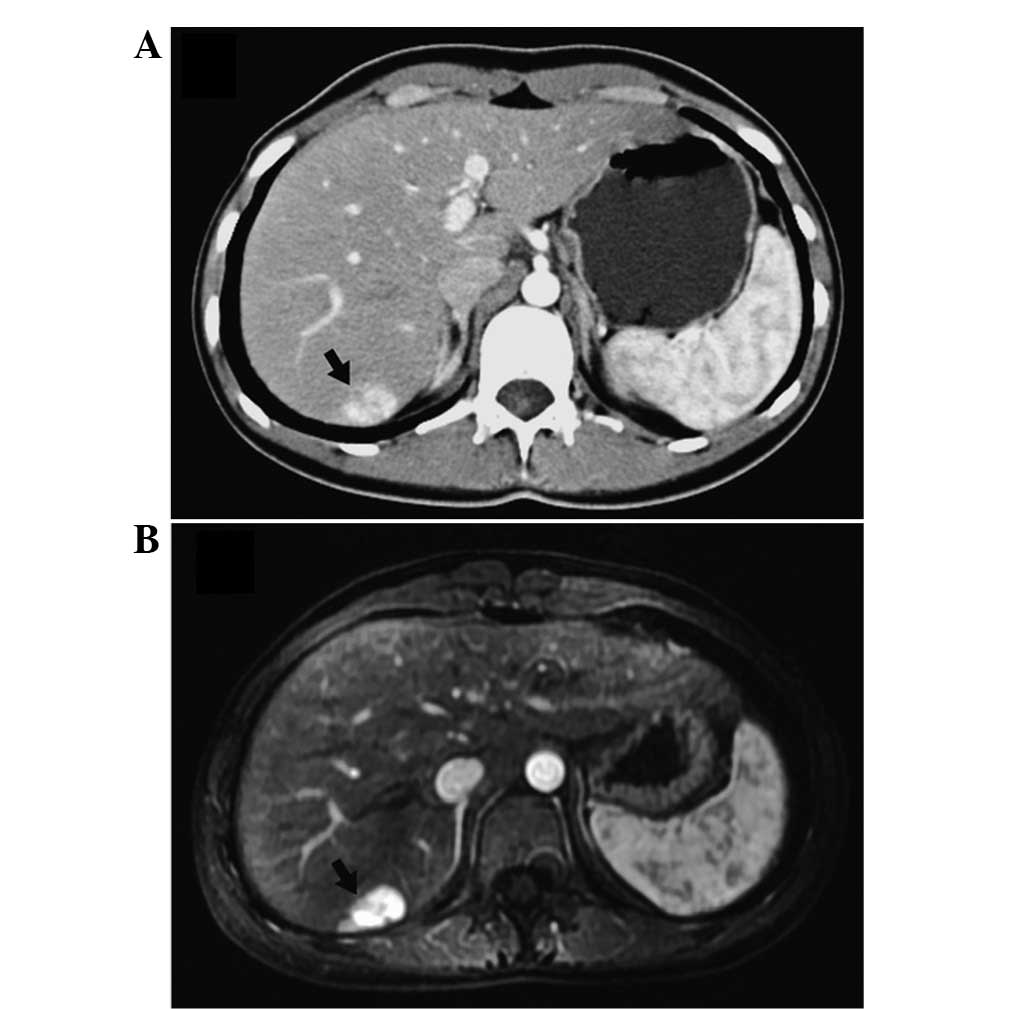
A plain computed tomography (CT) scan demonstrated
multiple lesions of low density with poorly-defined borders in
hepatic segments III (0.5×0.5 cm), IV (5.4×5.5 cm) and VII (1.8×1.5
cm). The delayed phase showed mild intensity lesions. However, the
intensity of the lesions increased significantly in the
contrast-enhanced phase (Fig. 1A).
A liver magnetic resonance imaging (MRI) scan revealed that the
lesions had a medium signal intensity on the T1-weighted image and
a slightly high signal on the T2-weighted image. The enhancement of
intensity of the lesions was also observed in the contrast-enhanced
phase of MRI (Fig. 1B).
Treatment
During the laparotomy, three well-encapsulated
tumors located in segment III, IV and VII were identified. No
portal or inferior vena cava vein invasion or distant metastasis
was observed. A partial hepatectomy of the liver neoplasms was
performed using the Pringle maneuver.
Pathology and immunohistochemical
analysis
The masses in segments III and IV were
pathologically identified as hemangioma, while the mass in segment
VII was revealed to be composed of polygonal morphology cells,
which are similar to epithelial cells. However, the latter mass did
not contain lipocytes or abnormal blood vessels.
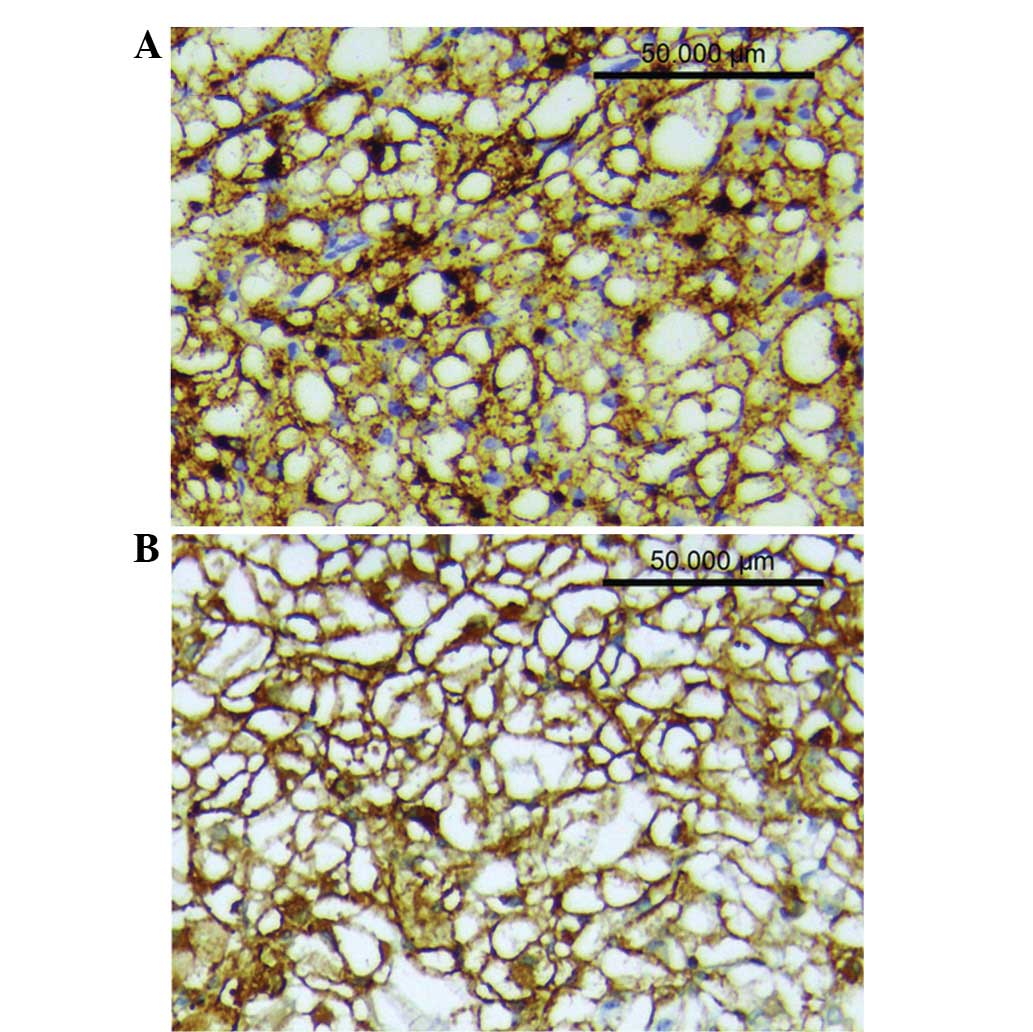
Immunohistochemistry further revealed that the mass in segment VII
was strongly positive for human melanoma black-45 (HMB-45; +++;
Fig. 2A), smooth muscle actin (SMA;
+++; Fig. 2B) and vimentin (++).
The mass was positive for CD34, but negative for S-100, creatine
kinase (CK), epithelial membrane antigen (EMA), desmin, AFP and
Ki67. A diagnosis of PEComa of the liver was confirmed based on the
immunohistochemical analysis. The patient recovered well and was
discharged one week after surgery. No evidence of recurrence was
observed during one year of follow-up.
Study approval
Approval for this study was obtained from the ethics
committee of Zhejiang University and informed consent was provided
by the patient.
Literature review
Identification of patients with
hepatic PEComa
The Chinese BioMedical Literature Database, the
China Hospital Knowledge Database and the Wanfangbase were searched
between January 2001 and December 2012. Repeated studies were
carefully screened and rejected from further analysis to avoid
over-representation. The final diagnosis of each case was confirmed
using pathological and immunohistochemical results. The data on the
clinical features, tumor characteristics, pre-operative imaging and
outcome of treatment of 19 cases were collected and analyzed along
with the data of the present case.
Presentation
The mean patient age was 43.4 years (range, 25–67
years) in the 20 patients. PEComa was shown to have a marked female
predominance (18 females and two males; Table I). The chief presenting complaints
were abdominal pain (5/20), abdominal discomfort (5/20) and
abdominal distension (1/20). Of the 20 patients, nine were
asymptomatic and discovered the mass incidentally during a physical
examination. The majority of the tumors were localized in the right
lobe (16/20) of the liver. The tumor size ranged between 2.0×1.6 cm
and 15.0×12.0 cm. Of the 20 tumors that were analyzed, seven were
>5 cm in size at the time of presentation.
 | Table IClinical data of 20 cases. |
Table I
Clinical data of 20 cases.
| First author, year
(ref.) | Gender/age,
years | Symptom | Size, cm | Location, lobe |
|---|
| Present case | F/25 | None | 2.5×1.0 | Left |
| Qiu et al,
2008 (19) | F/67 | Abdominal pain | 15.0×12.0 | Right |
| Deng et al,
2011 (20) | M/66 | None | 3.0×3.5 | Left |
| He et al, 2011
(21) | F/35 | None | 3.5×3.0 | Right |
| Han et al,
2008 (22) | M/44 | None | 2.0×1.6 | Right |
| Li et al, 2007
(23) | F/56 | Abdominal
distension | 5.0×4.0 | Left |
| Chen and Li, 2009
(24) | F/37 | Abdominal pain | 5.0×4.0 | Right |
| Zhang and Wang, 2012
(25) | F/55 | None | 3.0×3.0 | Right |
| Chen, 2009 (26) | F/36 | Abdominal pain | 7.0×5.0 | Right |
| Chen, 2009 (26) | F/45 | Abdominal
discomfort | 5.5×4.0 | Right |
| Liu et al,
2010 (27) | F/32 | None | 5.5×5.5 | Right |
| Zou et al,
2011 (28) | F/54 | Abdominal
discomfort | 6.0×5.0 | Right |
| Xu et al, 2001
(29) | F/35 | None | 2.0×2.0 | Right |
| Lin et al,
2002 (30) | F/30 | Abdominal
discomfort | 3.6×3.1 | Right |
| Liu et al,
2008 (31) | F/31 | Abdominal pain | 8.0×6.0 | Right |
| Zhu et al,
2010 (32) | F/26 | None | 5.0×3.0 | Right |
| Gao et al,
2012 (33) | F/59 | Abdominal pain | 6.0×5.0 | Right |
| Wang et al,
2007 (34) | F/46 | None | 4.0×4.0 | Right |
| Shi et al,
2010 (35) | F/41 | Abdominal
discomfort | 5.5×4.0 | Left |
| Shi et al,
2010 (35) | F/48 | Abdominal
discomfort | 8.0×6.0 | Right |
Pathological findings and
immunohistochemistry
Histological examination revealed that the tumor was
highly cellular, with large round or polygonal cells with abundant
cytoplasm and clear cell boundaries. Immunohistochemistry revealed
that the tumor cells in all cases were positive for HMB-45 (20/20)
and melan-A (9/9). The cells were positive for SMA (14/16),
vimentin (12/13) and S-100 (7/13) in the majority of the cases
(Table II).
| Table IIResults of the
immunohistochemistry. |
Table II
Results of the
immunohistochemistry.
|
Immunohistochemistry | Frenquency, %
(Positive cases/Total cases) |
|---|
| HMB-45 | 100 (20/20) |
| SMA | 88 (14/16) |
| Melan-A | 100 (9/9) |
| Vimentin | 92 (12/13) |
| S-100 | 54 (7/13) |
| Desmin | 40 (2/5) |
| CD34 | 45 (5/11) |
| AFP | 0 (0/10) |
| EMA | 0 (0/9) |
Treatment
All 20 patients underwent surgery following
admission. Three patients were treated with a hemihepatectomy,
three with a segmentectomy and 10 with a partial hepatectomy of the
liver neoplasms. However, no patients were administered
chemotherapy or radiotherapy.
Follow-up
The follow-up data was available for 14 patients and
the follow-up time ranged between 8 and 36 months. One patient
succumbed due to recurrence at two years post-surgery and the
others survived without recurrence or metastasis.
Discussion
The pathogenesis of PEComa, although discussed in
previous studies, remains controversial. Kenerson et
al(10) demonstrated that
tuberous sclerosis complex 1/2 (TSC1/2) inactivation and mTOR
hyperactivation were present in non-TSC AMLs and extrarenal PEComas
using immunohistochemistry and western blot analysis. In
particular, mTOR hyperactivation may be studied in such lesions
using immunohistochemical detection of p70S6K, which is a marker of
mTOR activity (6). Bing et
al(11) also showed that
epithelioid AMLs harbored p53 mutations in certain cases.
Hepatic PEComa occurs most commonly in females
(7), and symptoms of hepatic PEComa
usually show no specificity. In the present study, 11 out of 20
patients with hepatic PEComa had mild to significant non-specific
complaints. The remaining nine patients were asymptomatic. The
majority of the patients (16/20) had solitary lesions in the right
lobe, which was consistent with a previous study by Parfitt et
al(7).
Ultrasonograpy, CT and MRI are most frequently
employed for the pre-operative diagnosis of PEComa. Previous
studies have considered hypervascularity and arteriovenous
connections to be a feature of PEComa in contrast-enhanced CT
(8,12,13).
An MRI scan revealed that the PEComas were significantly and
heterogeneously enhanced in the arterial phase, but less enhanced
in the portal venous and delayed phases (14,15),
which may also effectively rule out a diagnosis of hepatocellular
carcinoma with a fibrotic capsule (15). Another commonly used diagnostic
method is contrast-enhanced ultrasonography, which possesses the
features of an early influx of the contrast agent into the tumor
and a rapid drainage of arterial blood to the veins (15). However, the accuracy of
pre-operative diagnosis is low, partly as a result of the variable
imaging appearances due to the varying proportion of the
components, including the smooth muscle cells, adipose tissue and
vessels, and the rarity of the tumor. In the present case, three
lesions of the liver shared similar imaging features, but only one
lesion was confirmed to be a PEComa. In the cases that were
reviewed in this study, three patients were pre-operatively
diagnosed with focal nodular hyperplasia (including the present
case), four patients were diagnosed with hepatic carcinoma and 12
patients could not be differentiated.
The final diagnosis of PEComa depends on the
pathology and immunohistochemistry. Martignoni et
al(6) defined PEComa as a tumor
that is composed of solely of cells with an epithelioid appearance,
which are closely associated with dilated vascular channels and
contain clear eosinophilic cytoplasms, but do not contain lipocytes
or disordered blood vessels. Almost all the PEComas were identified
to be strongly positive for melanocytic markers (HMB-45 and/or
melan-A) and smooth muscle markers (SMA and/or desmin) (2,5,16). In
the present study, the tumor cells of the 14 patients were positive
for HMB-45 and SMA, but in the case reported by Zou et
al(28), only HMB-45 and
melan-A were positive and SMA was not stained.
PEComa has been reported to exhibit benign behavior
in the majority of the literature. Since the first case of
malignant hepatic PEComa presented by Dalle et al(17), several malignant cases have been
reported (7,17,18).
In 2005, Folpe et al(16)
reviewed 26 cases of soft tissue and gynecological origins and
raised seven criteria to evaluate the malignancy of PEComa: i) A
tumor size of >5 cm; ii) infiltration into the surrounding
normal tissue; iii) a high nuclear grade; iv) hypercellularity; v)
high mitotic activity >1/50 high-power field); vi) coagulative
necrosis of the tumor; and vii) vascular invasion. A malignant
PEComa is considered to have two or more of the features that are
listed. Tumors with nuclear pleomorphisms, multinucleated giant
cells only or those of >5 cm in size are considered as neoplasms
of uncertain malignant potential. In the present study, one case of
malignant hepatic PEComa was also reviewed in which the patient was
identified to have a recurrence two years after the surgery.
Surgical resection with an adequate margin remains
the gold standard for the treatment of hepatic PEComa (6,9,14),
particularly in malignant cases. In the present study, all patients
underwent surgical treatment. The malignant patient underwent a
hemihepatectomy due to the enormous tumor size. Hemihepatectomies
were also performed in another two patients, who were misdiagnosed
with hepatocellular carcinoma prior to the surgery. Generally,
chemotherapy and radiotherapy does not indicate an improved
survival time (6). However, several
studies have shown promising treatment results, including a study
of rapamycin, which is an inhibitor for mTOR. Rapamycin had a
positive effect on renal angiomyolipoma (5). If rapamycin is able to yield the same
effect on other PEComas, this would provide the rationale for
lesions that are composed of PECs. Of the 14 patients in the
present study, 13 were alive during the 8–36-month follow-up period
and one succumbed due to recurrence. However, Parfitt et
al(7) noted that PEComa may
also demonstrate recurrence following a long period of time (nine
years). Thus, the prognosis of PEComa remains unpredictable, and it
is necessary to perform long-term follow-up studies for every
case.
In conclusion, the diagnosis of hepatic PEComa
depends on the pathological observations. Surgical resection of the
tumor appears to be necessary for a cure, particularly for
malignant tumors. Although adjuvant chemotherapy or radiotherapy
are not significant in the treatment, several studies that have
used drugs to treat PEComa have shown promising results. In the
present study, the tumors were mostly benign and the prognosis
following surgical resection was good.
Acknowledgements
This study was supported by the Foundation of
Science and Department of Technology, Zhejiang, China (no.
2011C13034-2).
References
|
1
|
Bonetti F, Pea M, Martignoni G and Zamboni
G: PEC and sugar. Am J Surg Pathol. 16:307–308. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Fletcher CD, Unni KK and Mertens F: World
Health Organization Classification of Tumors of Pathology and
Genetics: Tumors of Soft Tissue and Bone. 4. IARC Press; Lyon,
France: 2002
|
|
3
|
Folpe AL and Kwiatkowski DJ: Perivascular
epithelioid cell neoplasms: pathology and pathogenesis. Hum Pathol.
41:1–15. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Zamboni G, Pea M, Martignoni G, et al:
Clear cell ‘sugar’ tumor of the pancreas. A novel member of the
family of lesions characterized by the presence of perivascular
epithelioid cells. Am J Surg Pathol. 20:722–730. 1996.
|
|
5
|
Hornick JL and Fletcher CD: PEComa: what
do we know so far? Histopathology. 48:75–82. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Martignoni G, Pea M, Reghellin D, Zamboni
G and Bonetti F: PEComas: the past, the present and the future.
Virchows Arch. 452:119–132. 2008. View Article : Google Scholar
|
|
7
|
Parfitt JR, Bella AJ, Izawa JI and Wehrli
BM: Malignant neoplasm of perivascular epithelioid cells of the
liver. Arch Pathol Lab Med. 130:1219–1222. 2006.
|
|
8
|
Fang SH, Zhou LN, Jin M and Hu JB:
Perivascular epithelioid cell tumor of the liver: a report of two
cases and review of the literature. World J Gastroenterol.
13:5537–5539. 2007. View Article : Google Scholar
|
|
9
|
Strzelczyk JM, Durczynski A, Szymanski D,
Jablkowski M, Dworniak D and Sporny S: Primary perivascular
epithelioid cell tumor (PEComa) of the liver: report of a case.
Surg Today. 39:916–921. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Kenerson H, Folpe AL, Takayama TK and
Yeung RS: Activation of the mTOR pathway in sporadic
angiomyolipomas and other perivascular epithelioid cell neoplasms.
Hum Pathol. 38:1361–1371. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Bing Z, Yao Y, Pasha T, Tomaszewski JE and
Zhang PJ: p53 in pure epithelioid PEComa: an immunohistochemistry
study and gene mutation analysis. Int J Surg Pathol. 20:115–122.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Yamamoto H, Oda Y, Yao T, et al: Malignant
perivascular epithelioid cell tumor of the colon: report of a case
with molecular analysis. Pathol Int. 56:46–50. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Högemann D, Flemming P, Kreipe H and
Galanski M: Correlation of MRI and CT findings with histopathology
in hepatic angiomyolipoma. Eur Radiol. 11:1389–1395.
2001.PubMed/NCBI
|
|
14
|
Tan Y and Xiao EH: Hepatic perivascular
epithelioid cell tumor (PEComa): dynamic CT, MRI, ultrasonography,
and pathologic features - analysis of 7 cases and review of the
literature. Abdom Imaging. 37:781–787. 2012. View Article : Google Scholar
|
|
15
|
Akitake R, Kimura H, Sekoguchi S, et al:
Perivascular epithelioid cell tumor (PEComa) of the liver diagnosed
by contrast-enhanced ultrasonography. Intern Med. 48:2083–2086.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Folpe AL, Mentzel T, Lehr HA, Fisher C,
Balzer BL and Weiss SW: Perivascular epithelioid cell neoplasms of
soft tissue and gynecologic origin: a clinicopathologic study of 26
cases and review of the literature. Am J Surg Pathol. 29:1558–1575.
2005. View Article : Google Scholar
|
|
17
|
Dalle I, Sciot R, de Vos R, et al:
Malignant angiomyolipoma of the liver: a hitherto unreported
variant. Histopathology. 36:443–450. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Rouquie D, Eggenspieler P, Algayres JP,
Béchade D, Camparo P and Baranger B: Malignant-like angiomyolipoma
of the liver: report of one case and review of the literature. Ann
Chir. 131:338–341. 2006.PubMed/NCBI
|
|
19
|
Qiu ML, Liu JF, Zeng JH and Chen LH: Rare
epithelioid cell cancer around the liver blood vessels. Chin J
Hepatobil Surg. 14:18–41. 2008.(In Chinese).
|
|
20
|
Deng X, Qiu SS and Yang QC: Perivascular
epithelioid cell tumor of the liver: a report of one case and
review of the literature. Chin J Gen Surg. 20:99–101. 2011.(In
Chinese).
|
|
21
|
He GL, Pan MX, Gao Y, Cheng Y and Chen C:
Perivascular epithelioid cell tumor of the liver: a report of one
case. Chin J Practical Surg. 31:2682011.(In Chinese).
|
|
22
|
Han W, Jiang W, Li JS, Zhang ZT and Wang
N: Perivascular epithelioid cell tumor of the liver: a report of
one case and review of the literatur. Chin J Practical Surg.
28:556–558. 2008.
|
|
23
|
Li SY and Fang SH: Imaging diagnosis of
perivascular epithelioid cell tumor: report of two cases. J Med
Imaging. 17:1009–1010. 2007.(In Chinese).
|
|
24
|
Chen Y and Li JJ: One case: perivascular
epithelioid cell tumor of the liver. J Pract Radiol. 25:1614–1615.
2009.(In Chinese).
|
|
25
|
Zhang JG and Wang XM: A case of
perivascular epithelioid cell tumor of the liver on PET/CT. Chin J
Nucl Med Mol Imaging. 32:388–389. 2012.(In Chinese).
|
|
26
|
Chen JP: A clinicopathological study of
perivascular epithelioid cell tumor: report of two cases and review
of the literature. Jiangxi Med J. 44:1133–1134. 2009.(In
Chinese).
|
|
27
|
Liu J, Guo HX, Zhang L and Yuan L:
Perivascular epithelioid cell tumor of liver: clinicopathologic
observations. J Diag Pathol. 17:353–355. 2010.(In Chinese).
|
|
28
|
Zou XM, Shi Y and Li MW: Perivascular
epithelioid cell tumor of the liver: a report of one case. Chin J
Gen Surg. 20:604. 2011.(In Chinese).
|
|
29
|
Xu XY, Zhou XJ, Zhang T, Shi QL and Meng
K: Hepatic monotypic epithelioid angiomyolipoma: a case report and
literature review. J Clin Exp Pathol. 17:198–200. 2001.(In
Chinese).
|
|
30
|
Lin Y, Shi LQ, Zhou XJ, et al: Hepatic
monotypic epithelioid angiomyolipoma: two cases report and review
of literature. J Diag Pathol. 9:281–285. 2002.(In Chinese).
|
|
31
|
Liu ZJ, Yin P, Hong DX and Chen CC:
Hepatic epithelioid angiomyolipoma: a case report and literature
review. Chin J Clin Oncol. 35:775–776. 2008.(In Chinese).
|
|
32
|
Zhu PC, Yan F, Ma YL, Ao QL and Deng ZD:
Clinicopathologic features of epithelioid angiomyolipoma. Acta Med
Univ Sci Technol Huazhong. 39:528–531. 2010.(In Chinese).
|
|
33
|
Gao FP, Zhou XQ, Wei J, et al: Hepatic
epithelioid angiomyolipoma: a case report. Chin J Hepatobiliary
Surg. 18:345–376. 2012.(In Chinese).
|
|
34
|
Wang JF, Fan SF and Gan MF: Hepatic
epithelioid angiomyolipoma. Natl Med J Chin. 87:1839. 2007.(In
Chinese).
|
|
35
|
Shi QL, Hu Y, Xia H and Zhang XL:
Clinicopathologic diagnosis of Hepatic epithelioid angiomyolipoma.
Chin J Gen Surg. 25:493–494. 2010.(In Chinese).
|