Introduction
Angiosarcomas are rare, high-grade malignancies of
endothelial origin. The rarity of angiosarcomas makes clinical
diagnosis difficult. Histologically, angiosarcomas range from
well-differentiated tumors with variable endothelial atypia to
high-grade spindle cell neoplasms. Unlike the conventional
appearance, a particular morphological subtype of angiosarcoma, in
which the neoplastic endothelial cells have a predominantly
epithelioid character, has been termed epithelioid angiosarcoma
(EAS) (1). EAS most often arises in
the deep soft tissues of the extremities (2), but a variety of primary sites,
including the thyroid gland, skin, adrenal glands, gallbladder
(3), uterus (4), tonsil (5) and bone, have been reported (6). The pathological features of primary
renal EAS have been previously described in a study which used
fine-needle aspiration cytology (7). The present study reports a case of EAS
of the kidney that was diagnosed using resected tissue sections.
Based on its site of origin and the histological images, it is
necessary to distinguish EAS from other tumors of the kidney,
including metastatic carcinoma, melanoma and other epithelioid and
rhabdoid neoplasms. Immunohistochemical findings are useful for
diagnosing EAS. The patient provided written informed consent.
Case report
Patient presentation
A 75-year-old male presented at the Municipal
Hospital (Qingdao, China) with the chief complaint of recurrent
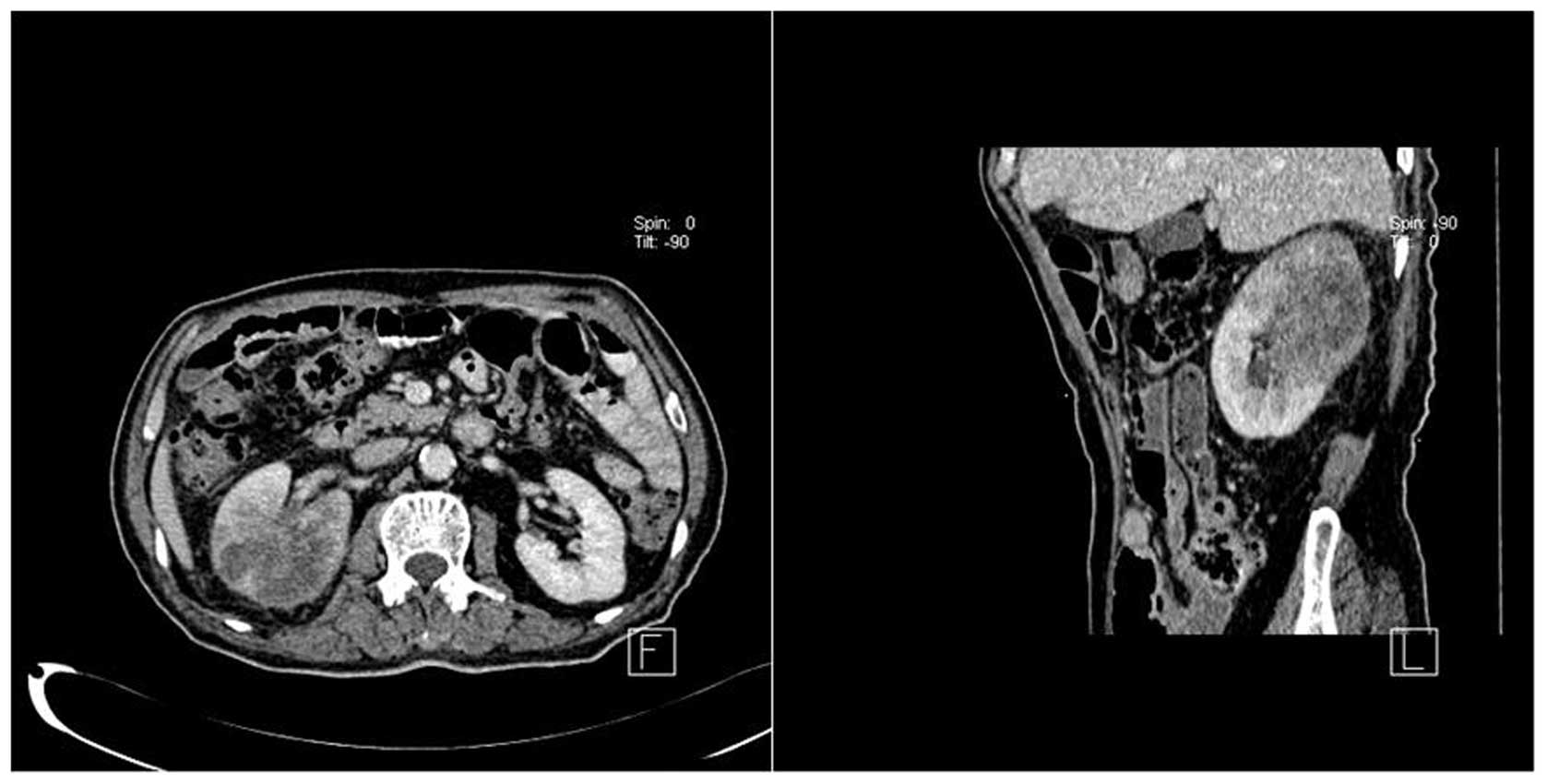
gross hematuria for approximately one month. An abdominal computed
tomography (CT) scan revealed space-occupying lesions in the
upper-mid section of the right kidney with mixed density (Fig. 1). No lesions were identified in the
other abdominal viscera or soft tissues. Renal cell carcinoma (RCC)
was suspected and the right kidney was resected.
Pathological findings
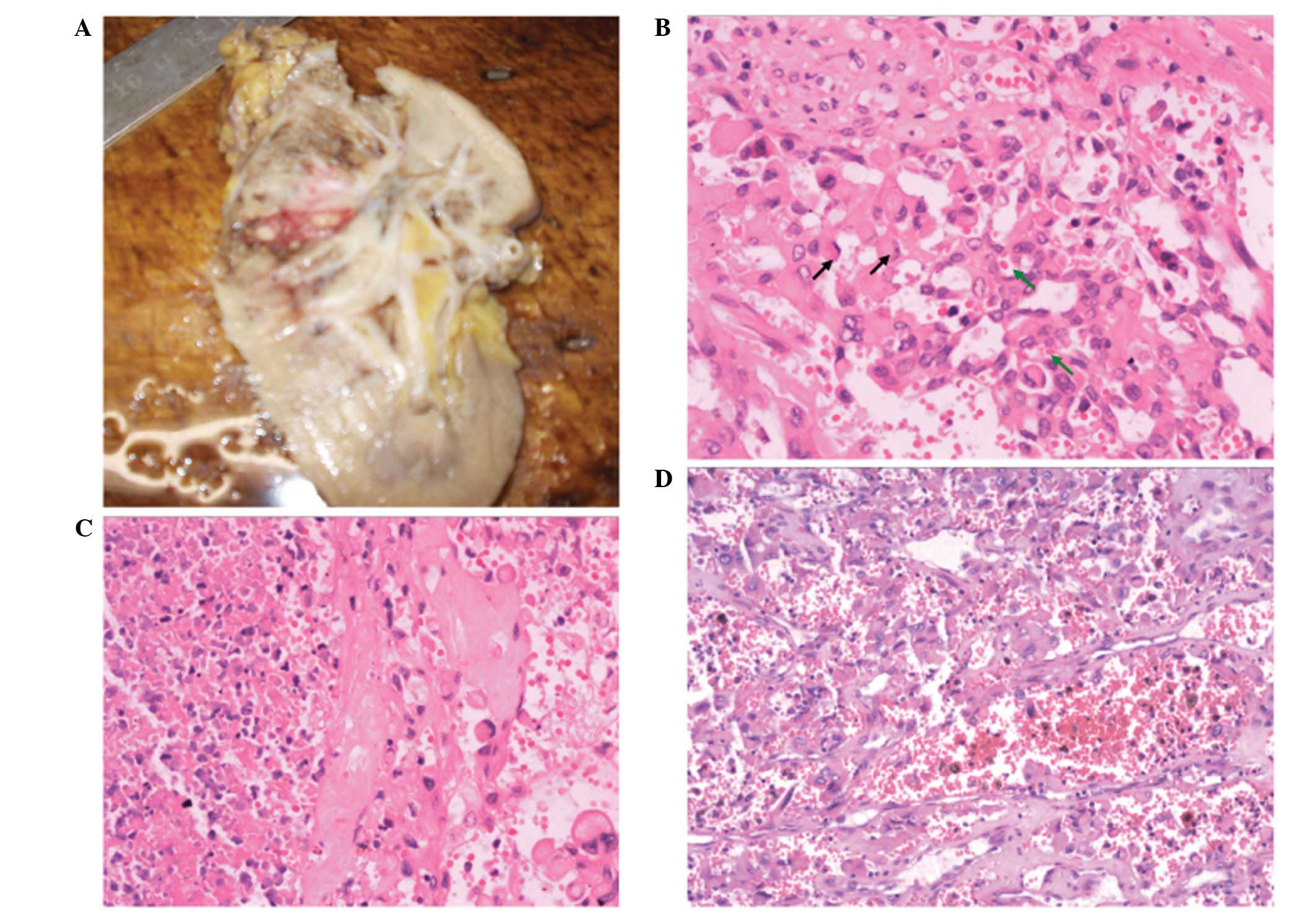
Grossly, the tumors presented as a large, necrotic,
hemorrhagic mass in the upper-mid section of the right kidney and
measured 4×4 cm in diameter (Fig.
2A). The poorly defined tumor margins extended close to the
renal capsule. Histopathology revealed large, mild-moderate
pleomorphic, round-polygonal epithelioid cells or spindle cells,
with vesicular nuclei containing prominent nucleoli. The malignant
endothelial cells were found to be filled with abundant
eosinophilic cytoplasm and certain cells appeared to mimic signet
ring cells. A few cells were observed to have intracytoplasmic
lumina containing erythrocytes, aiding the diagnosis (Fig. 2B). The cells were arranged in sheets
with extensive necrosis (Fig. 2C).
Focal areas of irregularly anastomosing vessel formation were also
present (Fig. 2D).
Immunohistochemistry was positive for AE1/AE3, cytokeratin (CK) 7,
vimentin, cluster of differentiation (CD) 31 and E-cadherin
(Fig. 3); however, no expression of
CD10, CD34, factor VIII, CK20, carcinoembryonic antigen (CEA) or
desmin was found. Staining for Ki-67 with MIB-1 was ~30%,
confirming the highly proliferative nature of these neoplasms.
Discussion
EAS has a male predilection and generally occurs in
adults, with the highest incidence in individuals in their seventh
decade (2). A number of clinical
presentations may be encountered due to diversity in the primary
sites of EAS. However, EAS of the kidney is particularly rare and
few clinical features have been described. In the present case, the
disease had developed insidiously and gross hematuria was the only
clinical manifestation. A CT scan revealed a space-occupying lesion
in the right kidney; however, the radiographic distinction between
RCC, AS and EAS is complex, as all of these neoplasms are highly
vascular and have large areas of necrosis (2).
The diagnosis of EAS primarily relies on
pathological examination. Brown et al (8) reported and reviewed 25 cases of renal
AS. Histologically, renal AS shows features similar to AS at other
sites. Renal AS is often poorly differentiated, thus the diagnosis
of renal AS requires the use of immunohistochemical methods to
distinguish it from other renal tumors that also have prominent
vascularity. Renal AS is positive for endothelial cell markers,
including CD31, CD34 and factor VIII, but negative for the
epithelial markers Cam 5.2, AE1/AE3 and EMA. A unique type of AS,
termed EAS has not been described in previous studies, with the
exception of a study which reported fine-needle aspiration cytology
of primary renal EAS (2). The
present study reported a case of EAS in the kidney which was
diagnosed using resected tissue sections. In previous cases,
immunostaining for factor VIII has been consistently positive among
cases of EAS, with stronger staining observed in malignant cells
compared with non-epithelioid vascular sarcomas (9). CD34 positivity has been reported to
range between 40 and 100%, and it typically stains in areas with
high vessel formation (9). In the
present case, the epithelioid tumor cells were found to be positive
for CD31, but negative for CD34 and factor VIII. Consequently, CD31
may be the most sensitive marker for identifying the poorly
differentiated endothelial cells. EAS is difficult to diagnose
using hematoxylin and eosin (H&E)-stained sections. In certain
cases, a sheeted epithelioid appearance and positive CK staining
make metastatic or primary carcinoma a strong diagnostic
consideration. Distinguishing features that are observed using
H&E analysis include areas of intracellular lumina, which may
or may not contain erythrocytes, revealing the endothelial nature
of EAS. The present case showed positive staining for AE1/AE3 and
CK7, but no staining for CK20 or CEA. Of note, the tumor cells were
found to be positive for E-cadherin which, to the best of our
knowledge, has not been previously reported in AS. With the
exception of primary and metastatic carcinoma, melanoma, malignant
mesothelioma, anaplastic large cell lymphoma, epithelioid sarcoma,
epithelioid hemangioendothelioma and malignant peripheral nerve
sheath tumor may exhibit histologic characteristics similar to EAS.
These tumors may be differentiated using a panel of
immunohistochemical stains (10–12).
In conclusion, the present study has reported a case
of EAS in the kidney and has reviewed findings from previous
studies. Although these soft tissue lesions most commonly occur at
other sites within the body, it is important that pathologists are
aware that they may also occur in the kidney. In the present case,
follow-up data suggested that early diagnosis may enhance
survival.
References
|
1
|
Fletcher CDM: Diagnostic Histopathology of
Tumors. 1. 3rd edition. Elsevier; Limited, Philadelphia, PA: pp.
66–67. 2007
|
|
2
|
Fletcher CDM, Beham A, Bekir S, Clarke AM
and Marler NJ: Epithelioid angiosarcoma of deep soft tissue: a
distinctive tumor readily mistaken for an epithelial neoplasm. Am J
Surg Pathol. 15:915–924. 1991.
|
|
3
|
Costantini R, Di Bartolomeo N, Francomano
F, Angelucci D and Innocenti P: Epithelioid angiosarcoma of the
gallbladder: case report. J Gastrointest Surg. 9:822–825. 2005.
|
|
4
|
Olawaiye AB, Morgan JA, Goodman A, Fuller
AF Jr and Penson RT: Epithelioid angiosarcoma of the uterus: a
review of management. Arch Gynecol Obstet. 278:401–404. 2008.
|
|
5
|
Agaimy A, Kirsche H, Semrau S, Iro H and
Hartmann A: Cytokeratin-positive epithelioid angiosarcoma
presenting in the tonsil: a diagnostic challenge. Hum Pathol.
43:1142–1147. 2012.
|
|
6
|
Meis-Kindblom JM and Kindblom LG:
Angiosarcoma of soft tissue: a study of 80 cases. Am J Surg Pathol.
22:683–697. 1998.
|
|
7
|
Singh C, Xie L, Schmechel SC, Manivel JC
and Pambuccian SE: Epithelioid angiosarcoma of the kidney: a
diagnostic dilemma in fine-needle aspiration cytology. Diagn
Cytopathol. 40(Suppl 2): E131–E139. 2012.
|
|
8
|
Brown JG, Folpe AL, Rao P, et al: Primary
vascular tumors and tumor-like lesions of the kidney: a
clinicopathologic analysis of 25 cases. Am J Surg Pathol.
34:942–949. 2010.
|
|
9
|
Jennings TA, Peterson L, Axiotis CA, et
al: Angiosarcoma associated with foreign body material. A report of
three cases. Cancer. 62:2436–2444. 1988.
|
|
10
|
Hart J and Mandavilli S: Epithelioid
angiosarcoma: a brief diagnostic review and differential diagnosis.
Arch Pathol Lab Med. 135:268–272. 2011.
|
|
11
|
Weed BR and Folpe AL: Cutaneous
CD30-positive epithelioid angiosarcoma following breast-conserving
therapy and irradiation: a potential diagnostic pitfall. Am J
Dermatopathol. 30:370–372. 2008.
|
|
12
|
Miettinen M, Fanburg-Smith JC, Virolainen
M, Shmookler BM and Fetsch JF: Epithelioid sarcoma: an
immunohistochemical analysis of 112 classical and variant cases and
a discussion of the differential diagnosis. Hum Pathol. 30:934–942.
1999.
|